
Metabolic heath: what to do to improve
Taking the pressure off insulin by eating a low carbohydrate diet can help with weight loss, metabolic health, insulin resistance and successfully put pre-diabetes and type 2 diabetes (T2D) into remission.
Sounds incredible but that’s what some people have been trying out for themselves and, for some, it seems to be working, although the numbers are still small.
Lowering carbohydrates essentially means cutting out starchy and high sugar food and drinks, which require the hormone insulin to process them, and replacing them with naturally nutrient-dense foods that are minimally altered from their natural state. The rationale behind this approach is that insulin is required to obtain energy from carbohydrates whereas fats and moderate quantities of protein don’t need insulin.
High insulin levels precede pre-diabetes and T2D, sometimes by more than 15 years. In one analysis, 50% of people (n= 2079) showed high insulin levels despite having normal glucose clearance. The majority of participants (93%) with impaired glucose tolerance or diabetes also had hyperinsulinaemia (raised insulin levels in the blood).
A low carbohydrate diet for better metabolic health
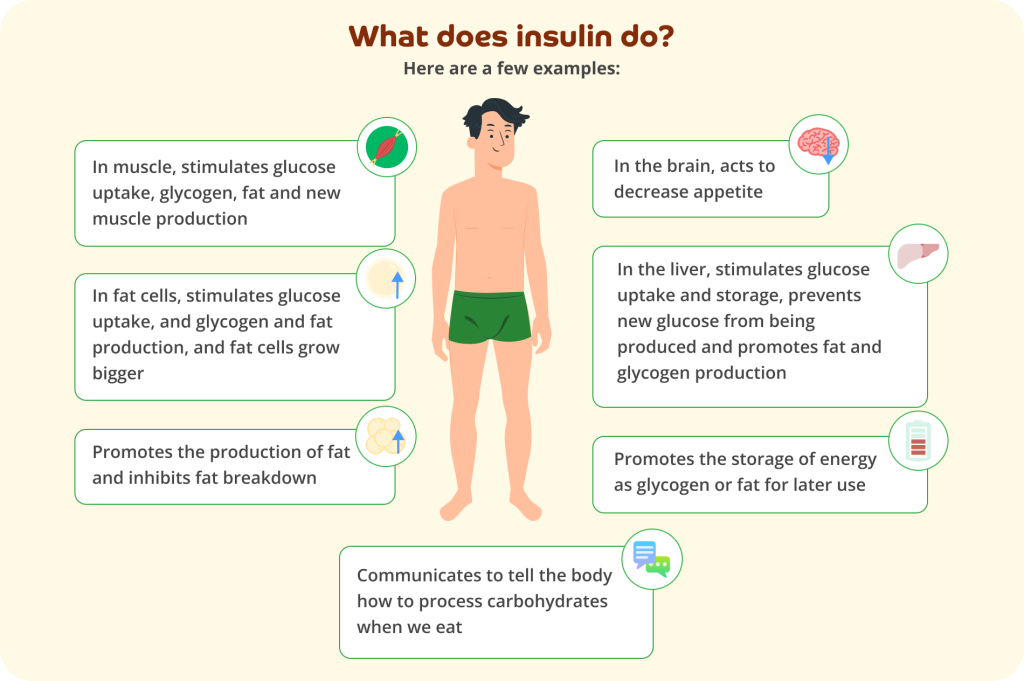
A lower carbohydrate diet (LCD) has been used successfully in 186 people in one GP practice over an average period of 33 months. Dr Unwin and his team at the Norwood GP Practice in Merseyside have published their findings. People lost an average of 8.9kg in weight and reduced their HbA1c (blood glucose levels) by an average of 17 mmol/mol. This was accompanied by better lipid (fatty acids) measurements and reductions in blood pressure.
51% of participants were able to come off their diabetes medication, effectively reversing their T2D. Diabetes remission was achieved in 77% of people who had been diagnosed with T2D for less than one year and in 20% of people who had been diagnosed for 15 years or more. In the study, diabetes remission was defined as no-longer having a diagnosis of T2D, including HbA1c less than 6.5% (48 mmol/mol), and not needing anti-diabetic medication. With less prescriptions for diabetes medications, it saved the NHS drugs budget £68,353 per year when compared to similar GP surgeries.
![Large brown text at the top says: 'Results of the Norwood surgery low carbohydrate programme' On the left is a yellow pie chart with smaller brown text above it saying: '51%'. Beneath it smaller grey text says: 'of participants were able to come off their diabetes medication.' Larger grey text beneath says: 'Diabetes remission was achieved in...' Below are two yellow pie charts. Above one on the left is a brown: '77%' and below that pie chart smaller grey text says: 'of people who has been diagnosed with type 3 diabetes for less than one year.' Slightly to the right above the second pie chart in brown text is says: '20%' and below the pie chart smaller grey text says: 'of people who had been diagnosed with type 2 diabetes for 15 years or more'. To the left is an illustration of a smiling Caucasian man with dark hair in green underwear. Next t him a three downwards brown arrows. Grey text next to the first arrow says: '8.9kg', grey text next to the second arrow says: 'HbA1c by 17mmol/mol' and grey text next to the third arrow says: 'Reduced blood pressure'. Beneath in a white box with curved corners grey text says: 'Saving the NHS drugs budget [in larger bold brown text] £68,353 [in normal large brown text] per year [in grey text] when compared to similar GP surgeries' All on a pale yellow background.](https://www.evergreen-life.co.uk/wp-content/uploads/2023/12/Results-of-the-Norwood-surgery-low-cabohyrdate-programme.png)
Haemoglobin A1c (HbA1c) is an important measure of how well blood glucose (sugar) is controlled. It gives an idea of the level of glucose (sugar) in the blood over a two-three month period.
People were monitored, given advice and information (educational and practical), such as how to deal with hurdles like low blood glucose and blood pressure changes. When a low carbohydrate diet is adopted, blood glucose levels typically fall significantly, as well as blood pressure. For this reason, diabetes medications need careful adjustment and ongoing guidance.
The lower carbohydrate diet sheet for T2D from Norwood surgery
If you have a long term condition or are on medication, please discuss with your GP before starting a low carbohydrate diet.
Low carbohydrate diets
Low carbohydrate diets are nothing new and there have been many versions in the literature, dating as far back as 160 years ago. Pioneers in the field of low carbohydrate diets, Jeff Volek and Stephen Phinney et al, showed back in 2008 in a randomised controlled trial of 40 overweight people with poor metabolic health, that a very low carbohydrate diet (in this case low enough to induce a measured mild ketosis – a sign that the body is burning fat) for a period of 12 weeks, had measurable benefits. These benefits included lowered fasting blood glucose (−12%) and insulin (−50%), lower insulin resistance (−55%), weight loss (−10%), decreased adiposity (−14%), and lowered triglycerides (−51%) when compared the group assigned to a low fat diet.
Despite the scale of the problem, published evidence for weight loss in problem areas such as T2D diabetes doesn’t support any particular one diet and most studies have been short – under one year. Recent analysis of low carbohydrate diets have struggled because the studies varied greatly in design and interpretation of “low carb.”
Overall, it’s being increasingly acknowledged that low carbohydrate diets can have important benefits for people with T2D, such as fewer blood glucose swings and reduced insulin secretion, reduced liver fat and lowered markers of inflammation. Also diets which include low glycaemic index (GI) foods rather than high-GI foods, have small but clinically useful effects on blood glucose control in patients with diabetes. The GI of a given food reflects how much its digestible carbohydrate content raises blood glucose levels. Low GI foods have a lower and slower impact on blood glucose. Further information on glycaemic index and glycaemic load (an extension of GI which takes portion size into account) can be found here.
There have been various interpretations of “low carbohydrate” in published studies:20-50g/day carbohydrates (less than 10% of the 2000 kcal/day) – low enough to induce ketosis often called a ketogenic diet or very low carb diet (VLCD). For example, the ketogenic diet is often composed of high fat (more than 90% fat by weight), low carbohydrates but adequate in protein, vitamins, and minerals; and is typically calorie restricted by 10%– 25%.
Less than 130g/day or less than 26% of the 2000 kcal/day diet and even less than 225g grams or less than 45% of the 2000 kcal/day diet (arguably not very low carb).
In the absence of a universally accepted definition, less than 130g per day of carbs per day is often used, with a focus on non-starchy vegetables and high fibre, low sugar fruits that are ideally less than 10g total carbohydrate per 100g weight.
It’s important to note that individuals respond to carbohydrates differently. One way to notice the impact of carbohydrates on blood sugar is to measure blood glucose; continuous blood glucose monitors can demonstrate in real time which foods are most problematic.
What is the difference between starches and sugars?
Starches are chains of single sugars – most often glucose – strung together. Starchy foods include bread, potatoes, pasta, rice, cereal and anything made of flours, such as wheat, corn (maize), barley.
Being essentially long chains of sugars, starches are very easily digested to sugars that look like this in structure:
As highlighted in the next graphic, starches are snipped up during digestion into single glucose molecules that are small enough for cells to absorb. The process of digesting starches begins in the mouth.
Carbohydrates and insulin
Insulin is produced in the pancreas and released into the upper digestive tract in response to raised blood glucose. It’s release is boosted when carbohydrate-sensing hormones come into contact with carbohydrates in the gut.
A high-carbohydrate diet which includes refined starchy foods (bread, potatoes, pasta, biscuits, cakes, crisps), and sugary foods (commonly found in low-fat foods), stimulates high insulin levels after eating.
Insulin travels in the blood and when it reaches the cells, it parks in various insulin specific parking places, called insulin receptors. Most all human cells have insulin receptors and respond to insulin.
Once insulin has docked, it causes an opening of the gates which allows glucose to enter inside the cell where it’s used for energy or converted for storage and later use. In health, the blood should hold around 4g of glucose (less than a teaspoon).
Insulin does much more than this but this is its most famous role (see below).
There are two main storage forms of glucose:
- Glycogen – a rapid release storage form, made from chains of linked glucose molecules
- Triglycerides (also known as tri-acylglycerol) – for longer term storage, excess glucose is converted into fat
Triglycerides are the main constituents of body fat in humans made from surplus energy.
Why are processed carbohydrates especially troublesome?
Processed carbohydrates are one of the smoking guns for insulin resistance because the processing alters the cellular structure of starches which makes them very easy to digest.
Under normal circumstances, hormones known as incretins sense carbohydrates as they travel along the upper part of the gut and send the signal that carbs are coming. This signals to the pancreas to release pre-made insulin into the blood in readiness to do its job, which is to move glucose into the cells. This happens in the upper part of the stomach.
When harder to digest carbs (coming from vegetables, for example) reach the lower intestine, counterbalancing hormones are released, which slows stomach emptying, giving rise to a sense of having eaten enough and stops further glucose from being released by the liver. This ensures carbs are processed in a controlled way in the lower gut.
However, if all the carbs are absorbed rapidly and easily and higher up (because the cellular structure which surrounds them has been destroyed in processing) the counterbalancing hormones aren’t activated and, as a result, causes damaging swings in blood glucose.
Adding fibre to a food doesn’t really help if the food also contains processed carbs, without their cellular structure, and therefore easily and rapidly digested.
Rather than be swayed by “with added fibre” messages on food labels, it’s best to check the total carbohydrate content per portion and per 100g. For comparison, a moderately low carbohydrate diet is considered to be less than 130g per day and “keto” is commonly below 50g per day.
Foods that come in a box or packaged with a barcode are also much more likely to be processed and to have a higher carbohydrate content.
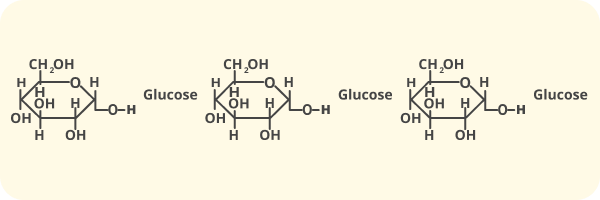
What does insulin do?
High insulin levels cause symptoms of tiredness, hunger, anxiousness, poor concentration, weight gain, sugar cravings, low motivation.
Overall, under conditions of high insulin levels it’s hard to burn fat for fuel. Even though there may be excess nutrients in the blood, because the insulin gates are closed, the cells and tissues may be deprived of energy.
Obesity
Since 1980, obesity has doubled in 73 countries and the rate of increase was even higher in children. It’s worth noting that not all obese people are metabolically unhealthy.
Obesity affects the poor disproportionately. The highest increase in obesity occurred in young men (25–29 years) in countries with a lower socio-economic index. Measurements of central obesity are linked with a higher risk of dying from all causes.
Things got quite a bit worse during the lockdown period, with a survey of 5000 people finding that 40% of individuals gained weight by an average of half a stone.
We cannot make vitamin D from sunlight here in the UK during winter, or get enough from food, and it’s really important for metabolic health. So, taking a supplement is recommended, although the dose you need is highly personal. People who are overweight often need higher doses.
What causes insulin to be raised?
When we eat carbohydrate insulin is released. Persistently high insulin is part of a complex cascade of effects which promotes energy storage, weight gain, hunger and low energy (lower metabolic rate). Increased consumption of refined carbohydrates and processed carbohydrates is an important contributing factor.
What causes insulin resistance?
High insulin causes insulin resistance and insulin resistance itself causes high insulin. The question is which comes first? Some think that over secretion of insulin in the B cells of the pancreas is the primary defect from which insulin resistance develops.
On the other hand, it has been shown experimentally that a constant infusion of insulin to healthy lean male volunteers induced insulin resistance within days – seen as insulin sensitivity falling by 20-40%. Resistance needs both high and persistent levels of insulin. Basically our bodies become deaf to a constant signal, which is only intended to last for a limited amount of time.
Other causes of insulin resistance include:
- Stress
- Oxidative stress
- Inflammation
- Infection, lipopolysaccharide, a dysfunctional gut microbiome
Insulin resistance is a description of a physiological state which can be reversed or put into remission.
How do you know if you have insulin resistance?
Measuring fasting insulin and something called a Homa-IR Index can help identify insulin resistance, which looks beyond blood glucose testing.
However, blood glucose measurements are more commonly used to identify whether your blood has unhealthy blood sugar levels. There are various ways to do this, including finger-prick testing and continuous blood glucose monitoring.
A fasting blood glucose test is usually taken after 8-10 hours without food or drink.
- Above 7 mmol/L indicates a diagnosis of diabetes
- Between 5.5 – 6.9 mmol/L indicates pre-diabetes
However, there are studies that suggest lower levels could be better.
In one large study of 46,578 people, a fasting blood glucose above 5 mmol/L (90 mg/dL) was associated with increased arterial stiffness. People with a fasting glucose levels of 5.28 – 5.5 mmol/L (95 to 99 mg/dL) were 2.33 times more likely to develop T2D compared with people who had a fasting plasma glucose levels less than 4.7 mmol/L (85 mg/dL).
We also know that that insulin is switched off when the level of glucose in the blood falls below 4.4-4.7 mmol/L (80-85 mg/dL). It’s a happy spot that might be a good place to aim for following a period of fasting.
Blood glucose testing is an indirect way of looking at insulin – high blood glucose is usually accompanied by high insulin (but not always) – that’s why insulin testing and sometimes C-peptide (which is a more stable measurement of insulin production) can provide specific information about insulin.
Fasting insulin, Homa-IR and C-peptide however, aren’t currently funded by the NHS. These alternative tests, can be important because insulin may be high even though blood glucose measurements are normal and it’s a way to notice insulin resistance earlier. Raised insulin levels can appear decades before raised blood glucose and HbA1c levels develop.
The results of any of these tests should be interpreted with the support of a suitably qualified health professional.
A few carbohydrate facts:
Farmers historically used to fatten animals for market by feeding them a combination of grains and skimmed milk, but they had to take care not to feed them too much of this carbohydrate-rich combination because to do so would make them too fat and unhealthy.
Sumo wrestlers maintain their huge body (average weight 100kg in one study) by eating a very high carbohydrate, low fat diet. They’re able to stay healthy whilst wrestling, but their metabolic fitness declines upon retirement. Their life expectancy is 10 years less than other Japanese people.
Cutting carbs is not new. Before insulin was discovered, it was the only way doctors had available to treat diabetes.
Other tips beyond a low carbohydrate diet
- Chew your food to allow your body time to sense and respond to the food you’re eating.
- Avoid snacking, particularly on carbohydrate containing snacks.
- Fasting/intermittent fasting allows insulin levels to fall and stored energy to be used.
Hurdles when embarking on a low carb diet
When starting on a low carbohydrate diet, blood glucose levels typically fall significantly, as does blood pressure. For this reason, prescribed medications may need careful adjustment and ongoing guidance.
Ensuring adequate electrolytes and hydration is recommended for people on low carb and ketogenic diets, especially if signs of low sodium, such as light-headedness, constipation, and headache develop.
Constipation can be prevented by increasing the amount of non-starchy green vegetables and high fibre vegetables and staying well hydrated.
Occasionally, people going low carb report episodes of gout. Usually the episodes are in the initial stages when the body is adjusting to the change of diet and tends to resolve as metabolic health improves. Some strategies include staying well hydrated, supporting bile production, sour cherries and citrus fruits for vitamin C (take care with fruits because of the sugar content), and avoiding alcohol.
Is a low carb diet suitable for me?
Cutting carbs has been shown to be beneficial for all kinds of people. However, if you do have a long-term medical condition, especially if you’re on long term medication, you should consult with your GP before embarking on a low-carb lifestyle, especially very low carbohydrate diets like a ketogenic diet. For example:
- Type 2 diabetes. While there is evidence to suggest a low carb, high fat diet might help lower blood sugar and reduce the risk of type 2 diabetes, a change in diet might change the effectiveness of certain diabetes medications.
- Those with high blood pressure. Taking medication for high blood pressure and using a low carb diet can put you at risk of low blood pressure within a matter of days, so consult your GP on how to manage this before starting.
- There are a few groups of people for whom keto might not be a good idea, such as chronic kidney disease (CKD).
- People undertaking high-level athletic training – best to discuss with a suitably qualified health professional, nutritionist or trainer.
- DNA signposts. A DNA test could tell you more about whether a KETO diet would work for you. For example, if you metabolise monounsaturated fats well and carbs not so quickly, then you’re likely to be suited to a more keto-style diet. Alternatively, a better metabolism of carbs but not fats could make you less suited to keto. Find out how well you’re likely to metabolise both of these with an Evergreen Life DNA Test.
If you have a long term condition or are on medication, please discuss with your GP before starting a low carbohydrate diet.
Long term concerns over the nutritional content of low carbohydrate diets
Low carbohydrate diets for six months can be used safely and may help towards remission of diabetes without adverse effects. This doesn’t mean that low carb diets longer term are unsafe, it’s just that there aren’t that many long term studies.
Most of the concerns surrounding low carbohydrate diets have stemmed from studies in epileptic children, many studies were short term and the studies varied greatly in diet quality. This makes it hard to draw meaningful conclusions and comparisons.
Summary
There are many different interpretations of “low carbohydrate” diets and various definitions of “low carbohydrate.” Some specify keeping carbohydrates within tight boundaries. Other groups have also included calorie restriction.
In general, the degree of carbohydrate restriction necessary depends on the person, their situation/starting point, their goals and how intolerant to carbohydrates/insulin resistant they are. Some people will need to be stricter.
In the diet recommended by Dr Unwin, most of the foods that are restricted are high in sugars and starches. These are replaced by naturally nutrient-dense foods which includes unlimited amounts of green vegetables and salads.
In Dr Unwin’s study, the group of people that had the greatest success were those newly diagnosed with T2D (duration less than one year) compared to those diagnosed for longer (15 years or more). It’s not a surprise because chronically high blood glucose, insulin resistance and poor metabolic health causes increasing and progressive damage which, if not corrected, at some point may become increasingly irreversible.
However, it’s never to late to try and all the more reason to start sooner.
Further help, information and resources can be found at the Public Health Collaboration here or contact your GP for advice.

Reviewed by:
Anna Keeble MA BA Head of Content and Wellbeing Expert
Dr Claire Marie Thomas MRCGP DFSRH DTMH DipNLP MBChB BMedSci Medical Expert
- Abdul-Ghani, M. and DeFronzo, R.A. (2021). Insulin Resistance and Hyperinsulinemia: the Egg and the Chicken. The Journal of Clinical Endocrinology & Metabolism 106(4) 1987-1899. Available here.
- Banting, W. (1993). Letter on Corpulence, Addressed to the Public. Obesity Research, [online] 1(2), pp.153–163. Available here.
- BBC (2021). Lockdown weight gain averaging half a stone – survey. BBC News. [online] 26 Jul. Available here. [Accessed 21.Dec 2023].
- Bough, K. (2008). Energy metabolism as part of the anticonvulsant mechanism of the ketogenic diet. Epilepsia, 49, pp.91–93. Available here.
- Brand-Miller, J., Hayne, S., Petocz, P. and Colagiuri, S. (2003). Low-Glycemic Index Diets in the Management of Diabetes: A meta-analysis of randomized controlled trials. Diabetes Care, [online] 26(8), pp.2261–2267. Available here.
- Browning, J.D., Baker, J.A., Rogers, T., Davis, J., Satapati, S. and Burgess, S.C. (2011). Short-term weight loss and hepatic triglyceride reduction: evidence of a metabolic advantage with dietary carbohydrate restriction. The American Journal of Clinical Nutrition, [online] 93(5), pp.1048–1052. Available here.
- Chan, K.L., Cathomas, F. and Russo, S.J. (2019). Central and Peripheral Inflammation Link Metabolic Syndrome and Major Depressive Disorder. Physiology, 34(2), pp.123–133. Available here.
- Chakaroun, R.M., Massier, L. and Kovacs, P. (2020). Gut Microbiome, Intestinal Permeability, and Tissue Bacteria in Metabolic Disease: Perpetrators or Bystanders? Nutrients, [online] 12(4), p.1082. Available here.
- Christou, M.A., Christou, P.A., Kyriakopoulos, C., Christou, G.A. and Tigas, S. (2023). Effects of Hypoglycemia on Cardiovascular Function in Patients with Diabetes. International Journal of Molecular Sciences, [online] 24(11), p.9357. Available here.
- Churuangsuk, C., Hall, J., Reynolds, A., Griffin, S.J., Combet, E. and Lean, M.E.J. (2022). Diets for weight management in adults with type 2 diabetes: an umbrella review of published meta-analyses and systematic review of trials of diets for diabetes remission. Diabetologia, 65(1),pp.14-36. Available here.
- Crofts, C., Schofield, G., Zinn, C., Wheldon, M. and Kraft, J. (2016). Identifying hyperinsulinaemia in the absence of impaired glucose tolerance: An examination of the Kraft database. Diabetes Research and Clinical Practice, 118, pp.50–57. Available here.
- Crowe, T.C. (2005). Safety of low-carbohydrate diets. Obesity Reviews, 6(3), pp.235–245. Available here.
- Del Prato, S., Leonetti, F., Simonson, D.C., Sheehan, P., Matsuda, M., and DeFronzo, R.A. (1994) Effect of sustained physiologic hyperinsulinaemia and hyperglycaemia on insulin secretion and insulin sensitivity in man. Diabetologia 37: 1025-1035. Available here.
- Diabetes.co.uk (2023). A C-peptide test is a blood test which is carried out to find out how much insulin your body is producing. [online] Diabetes. Available here. [Accessed 21 Nov. 2019].
- Diabetes.co.uk. (2019). Hyperinsulinemia – Causes, Risks & Hyperinsulinemia Symptoms. [online] Available here. [Accessed 21.Dec 2023].
- Diabetes UK (n.d.). Diabetes and Checking Your Blood Sugars. [online] Diabetes UK. Available here. [Accessed 21.Dec 2023].
- Diabetes UK (n.d.). Low-carb diet and meal plan. [online] Diabetes UK. Available here. [Accessed 21.Dec 2023].
- Diabetes UK and SACN (2021) Lower carbohydrate diets for adults with type 2 diabetes. [online] Available here. [Accessed 21. Dec 2023].
- Goldenberg, J.Z., Day, A., Brinkworth, G.D., Sato, J., Yamada, S., Jönsson, T., Beardsley, J., Johnson, J.A., Thabane, L. and Johnston, B.C. (2021). Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission: systematic review and meta-analysis of published and unpublished randomized trial data. BMJ, [online] 372(372), p.m4743. Available here.
- Haeusler, R.A., McGraw, T.E. and Accili, D. (2017). Biochemical and cellular properties of insulin receptor signalling. Nature Reviews Molecular Cell Biology, [online] 19(1), pp.31–44. Available here.
- Hallberg, S.J., McKenzie, A.L., Williams, P.T., Bhanpuri, N.H., Peters, A.L., Campbell, W.W., Hazbun, T.L., Volk, B.M., McCarter, J.P., Phinney, S.D. and Volek, J.S. (2018). Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. Diabetes Therapy, [online] 9(2), pp.583–612. Available here.
- Hallberg, S.J., Gershuni, V.M., Hazbun, T.L. and Athinarayanan, S.J. (2019). Reversing Type 2 Diabetes: A Narrative Review of the Evidence. Nutrients, [online] 11(4), p.766. Available here.
- Hoehn, K.L., Salmon, A.B., Hohnen-Behrens, C., Turner, N., Hoy, A.J., Maghzal, G.J., Stocker, R., Van Remmen, H., Kraegen, E.W., Cooney, G.J., Richardson, A.R. and James, D.E. (2009). Insulin resistance is a cellular antioxidant defense mechanism. Proceedings of the National Academy of Sciences of the United States of America, [online] 106(42), pp.17787–92. Available here.
- Holst, J.J. (2019). The incretin system in healthy humans: The role of GIP and GLP-1. Metabolism, 96, pp.46–55. Available here.
- Jayedi, A., Soltani, S., Zargar, M.S., Khan, T.A. and Shab-Bidar, S. (2020). Central fatness and risk of all cause mortality: systematic review and dose-response meta-analysis of 72 prospective cohort studies. BMJ, p.m3324. Available here.
- Jeong, I.-K. (2012). The Role of Cortisol in the Pathogenesis of the Metabolic Syndrome. Diabetes & Metabolism Journal, 36(3), p.207-210. Available here.
- Kelley, D., Adkins, Y. and Laugero, K. (2018). A Review of the Health Benefits of Cherries. Nutrients, [online] 10(3), p.368. Available here.
- Kronenberg, F., Mora, S., Stroes, E.S.G., Ference, B.A., Arsenault, B.J., Berglund, L., Dweck, M.R., Koschinsky, M., Lambert, G., Mach, F., McNeal, C.J., Moriarty, P.M., Natarajan, P., Nordestgaard, B.G., Parhofer, K.G., Virani, S.S., von Eckardstein, A., Watts, G.F., Stock, J.K. and Ray, K.K. (2022). Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. European Heart Journal, 43(39), pp.3925–3946. Available here.
- Liang, H., Hussey, S.E., Sanchez-Avila, A., Tantiwong, P. and Musi, N. (2013). Effect of Lipopolysaccharide on Inflammation and Insulin Action in Human Muscle. PLoS ONE, 8(5), p.e63983. Available here.
- Ludwig, D.S., Aronne, L.J., Astrup, A., de Cabo, R., Cantley, L.C., Friedman, M.I., Heymsfield, S.B., Johnson, J.D., King, J.C., Krauss, R.M., Lieberman, D.E., Taubes, G., Volek, J.S., Westman, E.C., Willett, W.C., Yancy, W.S. and Ebbeling, C.B. (2021). The carbohydrate-insulin model: a physiological perspective on the obesity pandemic. The American Journal of Clinical Nutrition, 114(6), pp.1873-1885. Available here.
- Murdoch, C., Unwin, D., Cavan, D., Cucuzzella, M. and Patel, M. (2019). Adapting diabetes medication for low carbohydrate management of type 2 diabetes: a practical guide. British Journal of General Practice, [online] 69(684), pp.360–361. Available here.
- Nichols, G.A., Hillier, T.A. and Brown, J.B. (2008). Normal Fasting Plasma Glucose and Risk of Type 2 Diabetes Diagnosis. The American Journal of Medicine, [online] 121(6), pp.519–524. Available here.
- Nishizawa, T., Akaoka, I., Nishida, Y., Kawaguchi, Y., Hayashi, E. and Yoshimura, T. (1976). Some factors related to obesity in the Japanese sumo wrestler. The American Journal of Clinical Nutrition, 29(10), pp.1167–1174. Available here.
- Oliver, A.W., Potter, E.L. and Oregon State Agricultural College Agricultural Experiment Station (1930) Fattening pigs for market. Agricultural Experiment Station, Oregon State Agricultural College. Available here.
- Pais, R., Gribble, F.M. and Reimann, F. (2015). Stimulation of incretin secreting cells. Therapeutic Advances in Endocrinology and Metabolism, 7(1), pp.24–42. Available here.
- Public Health Collaboration. (n.d.). Healthy Eating Guidelines & Weight Loss Advice For The UK – Public Health Collaboration. [online] Available here. [Accessed 21 Dec. 2023].
- Public Health Collaboration. (n.d.). Resources – Public Health Collaboration. [online] Available here. [Accessed 21 Dec. 2023].
- Public Health Collaboration. (n.d.). The One Page Diet Sheet Courtesy Of Dr David Unwin – Public Health Collaboration. [online] Available here.
- Riddle, M.C., Cefalu, W.T., Evans, P.H., Gerstein, H.C., Nauck, M.A., Oh, W.K., Rothberg, A.E., le Roux, C.W., Rubino, F., Schauer, P., Taylor, R. and Twenefour, D. (2021). Consensus Report: Definition and Interpretation of Remission in Type 2 Diabetes. Diabetes Care, 44(10), pp.2438–2444. Available here.
- Rizza, R.A., Mandarino, L.J., Genest, J., Baker, B.A. and Gerich, J.E. (1985). Production of insulin resistance by hyperinsulinaemia in man. Diabetologia, [online] 28(2), pp.70–75. Available here.
- Saklayen, M.G. (2018). The Global Epidemic of the Metabolic Syndrome. Current Hypertension Reports, [online] 20(2):12. Available here.
- Samkani, A., Skytte, M.J., Kandel, D., Kjaer, S., Astrup, A., Deacon, C.F., Holst, J.J., Madsbad, S., Rehfeld, J.F., Haugaard, S.B. and Krarup, T. (2018). A carbohydrate-reduced high-protein diet acutely decreases postprandial and diurnal glucose excursions in type 2 diabetes patients. British Journal of Nutrition, 119(8), pp.910–917. Available here.
- Scazzina, F., Siebenhandl-Ehn, S. and Pellegrini, N. (2013). The effect of dietary fibre on reducing the glycaemic index of bread. British Journal of Nutrition, 109(7), pp.1163–1174. Available here.
- Unwin, D., Delon, C., Unwin, J., Tobin, S. and Taylor, R. (2023). What predicts drug-free type 2 diabetes remission? Insights from an 8-year general practice service evaluation of a lower carbohydrate diet with weight loss. BMJ Nutrition, Prevention & Health, [online] 6(1), p.e000544. Available here.
- Unwin, D., Khalid, A.A., Unwin, J., Crocombe, D., Delon, C., Martyn, K., Golubic, R. and Ray, S. (2020). Insights from a general practice service evaluation supporting a lower carbohydrate diet in patients with type 2 diabetes mellitus and prediabetes: a secondary analysis of routine clinic data including HbA1c, weight and prescribing over 6 years. BMJ Nutrition, Prevention & Health, [online] 3(2), pp.285-294. Available here.
- Vecchio, I., Tornali, C., Bragazzi, N.L. and Martini, M. (2018). The Discovery of Insulin: An Important Milestone in the History of Medicine. Frontiers in Endocrinology, [online] 9(613). Available here.
- Volek, J.S., Phinney, S., Forsythe, C., and Quann, E.E. (2009.) Carbohydrate Restriction has a More Favorable Impact on the Metabolic Syndrome than a Low Fat Diet. Lipids, 44(4):297-309. Available here.



