
In today’s sun-exposed world, the prevalence of skin cancer continues to rise, making it essential to recognise its signs early on. Understanding what skin cancer looks like and when to seek medical attention is needed for early detection and successful treatment. In this comprehensive guide, we’ll explore the different types of skin cancer, their different characteristics, the ABCDEs of skin cancer evaluation and when it’s time to consult your GP.
The importance of skin cancer awareness
According to Cancer Research UK, rates of skin cancer are increasing year on year and are the most common form of cancer in the UK. This may be linked to rising temperatures and people wishing to make the most out of the summer sun and using sunbeds. Ultraviolet (UV) radiation is a main risk factor for skin cancer and overexposure to UV is associated with 9 out of 10 diagnoses of all skin cancers in the UK.
All cells in the body need to divide and replicate in order for us to live. The problem arises when cells become damaged and start to mutate. Over time, UV rays can damage the DNA in skin cells, leading them to divide and grow uncontrollably. This is the basis of cancer formation.
However, UV stimulates the skin to produce vitamin D which is an essential micronutrient for health throughout all life stages. Therefore, achieving a healthy balance of sunlight is important. Our article on keeping your skin healthy inside and out covers the question: How much sunshine do I need for enough vitamin D and to avoid skin cancer?
Skin cancer rates are more prevalent in the UK among white individuals. However, people of black and other minority ethnic backgrounds should still take precautions and protect their skin. In fact, sadly, despite lower incidences of skin cancers among black people, diagnoses are often made later on those with black and brown skin than on those with lighter skin, often leading to a poorer outcomes. A study on skin cancer risk perceptions suggests that this may be partly due to individuals with darker skin tones thinking of themselves as having a lower risk.
Ageing skin is also another risk factor for skin cancer development. As a whole, we are living longer, and so some of the rising trends in skin cancer can be linked to the UK’s growing, ageing population.
Types of skin cancer
There are two main forms of skin cancer: melanoma and non-melanoma and these can be further subdivided. Different skin cancer types refer to the specific cells within the skin that are affected. We will look in closer detail at cancers affecting basal cells, squamous cells and melanocytes.
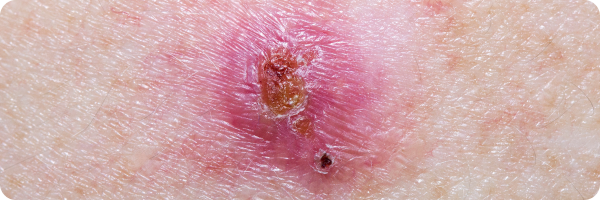
Basal cell carcinoma
Basal cell carcinomas (BCC) are the most common type of non-melanoma skin cancer, accounting for around 75% of all skin cancer cases. They originate in the basal cells, which are responsible for producing new skin cells as old ones die off.
Symptoms:
BCC usually develops on sun-exposed areas, such as the face, head, neck and shoulders, but can appear anywhere on the body.
- Open sore:
- An unhealed sore that may bleed, ooze, or crust.
- It can persist for weeks or appear to heal and then recur.
- Reddish patch or irritated area:
- Found on the face, chest, shoulder, arm, or leg.
- May crust, itch, hurt, or cause no discomfort.
- Shiny bump or nodule:
- Can be pearly, clear, pink, red, or white.
- In people of colour, it might also appear tan, black, or brown.
- Sometimes mistaken for a normal mole.
- Small pink growth:
- Has a slightly raised, rolled edge.
- Features a crusted indentation in the centre.
- May develop tiny surface blood vessels over time.
- Scar-like area:
- Appears flat, white, yellow, or waxy.
- Skin looks shiny and taut.
- Often has poorly defined borders.
- This sign could indicate an invasive BCC.
For examples of BCCs, the Skin Cancer Foundation showcases lots of different presentations.
Disclaimer: The skin cancer images are for educational purposes only and the appearance of skin cancer can vary widely from person to person. The images should not be used as a substitute for professional medical diagnosis or advice.
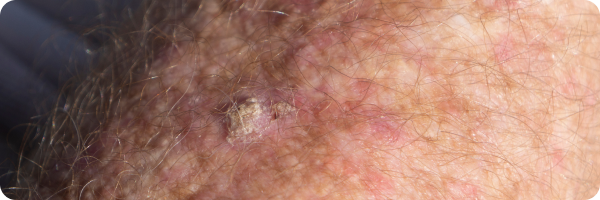
Squamous cell carcinoma
Squamous cell carcinomas (SCCs) occur in the outermost layer of skin which is also called the epidermis. This layer is made up of squamous cells which form a barrier to the underlying tissues, protecting them from damage, infection and dehydration.
Symptoms:
SCC can develop anywhere but are most common on sun-exposed areas, such as the lips, scalp, back of hands, forearms, ears, face, etc. They can also develop in scars, sores and sites of skin injury and the skin around the lesion can often indicate sun damage: the surrounding skin may have wrinkles, changes in pigment or feel less elastic.
SCCs can vary in appearance but may appear as:
- Thick, scaly, rough areas of skin prone to crusting or bleeding.
- Similar appearance to warts.
- Persistent open sores that resist complete healing.
- Elevated growths with a central depression, that can lead to itching or bleeding.
Images of SCC can be found on the British Skin Foundation website.
Disclaimer: The skin cancer images are for educational purposes only and the appearance of skin cancer can vary widely from person to person. The images should not be used as a substitute for professional medical diagnosis or advice.
Melanomas
Melanomas affect melanocytes which are the cells responsible for producing melanin, the pigment that gives skin its colour. Melanin helps protect the skin against UV rays and increases with sun exposure. While melanomas are more common in sun-exposed areas, especially for those with lighter skin, they can occur anywhere.
Although everyone has a similar number of melanocytes, individuals with brown or black skin have more active melanocytes, producing more melanin, resulting in higher pigment levels. Rarely, melanomas can develop in non-sun-exposed areas. This is particularly true of acral melanomas which often affect the nails, palms and soles of the feet. Acral melanomas are diagnosed at a high proportion in people with brown or black skin.
In the UK, melanoma is the 5th most common cancer. Though less prevalent than BCC and SCC, this skin cancer poses a greater threat due to its ability to spread rapidly to other organs when not promptly treated in its early stages.
Symptoms:
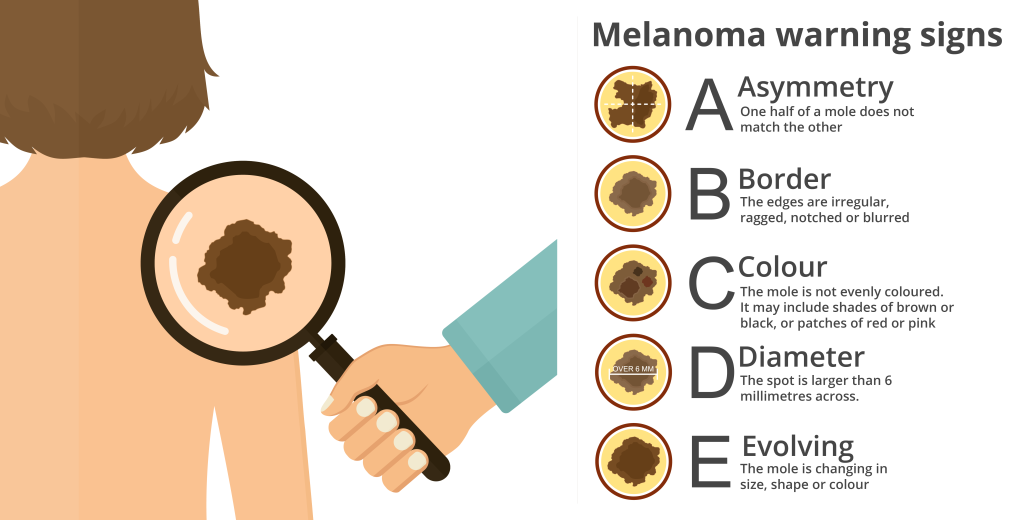
Melanomas can develop on any part of the body, whether that be a patch of normal skin, a mole, the palms, the soles of the feet or under the nails. Although they are more common on the back, legs, arms and face, they are most commonly related to the appearance of a new mole or changes to a mole you already have. To aid in identifying potential signs of melanoma, the ABCDE rule can serve as a helpful guide when checking moles:
Cancer Research UK provides some pictures of melanomas, changes to skin and abnormal moles.
Disclaimer: The skin cancer images are for educational purposes only and the appearance of skin cancer can vary widely from person to person. The images should not be used as a substitute for professional medical diagnosis or advice.
Risk factors
Although skin cancer can vary in type, they share some common risk factors. BCC, SCC and melanoma can all be influenced by:
- Excessive UV exposure: BCCs, SCCs and melanomas are often linked to sun/sunbed damage and long-term overexposure to UV rays. This is especially true among fair-skinned people and those who work outdoors or spend a lot of leisure time in the sun. Melanoma risk goes up alongside increasing sunburns throughout all life stages, not just childhood.
- Increasing age: BCC and SCC are more common as people get older. Melanomas are a little different as they can affect any age and are frequently seen in patients under 55, with 75% of melanoma diagnoses are in those under aged 70.
- Past history, family history and genetics: A genetic predisposition to skin cancer can increase one’s risk. Those who have already had skin cancer (melanoma or non-melanoma) or have a family member who has had melanoma is at an increased risk of developing melanoma. A history of BCC or the human papilloma virus can increase the risk of developing SCC.
- Number of moles: Having a large number of moles increases the risk of melanoma as there is a greater likelihood of developing abnormal moles or for changes to occur to existing moles.
- Presence of skin precancers: Precancers, like actinic keratosis, may account for 40-60% of SCCs origins.
- Sex: BCC, SCC and melanoma appears to be more common among men than women.
- Certain medications: Long-term use of medications that suppress the immune system or individuals with a compromised immune system appear to have an increased risk of BCC, SCC and melanoma.
If you think you may be at an increased risk due to any of the above factors, it’s especially important to check your skin regularly and report any changes early to your healthcare provider.
Treatment and prognosis
Despite how common they are, BCCs are slow-growing and generally respond very well to treatment, especially when diagnosed early. Most cases of SCC are also considered low-risk if detected early. Melanoma is a more aggressive form of cancer and may require urgent referral to a specialist. The prognosis depends on the stage of the melanoma.
Surgery is the primary treatment of all skin cancers, but especially for SCC and melanoma, particularly malignant melanoma. Malignant melanoma is a more aggressive type of cancer and requires rapid detection and treatment to try to prevent it from spreading. Radiotherapy, targeted medicines, immunotherapy, and chemotherapy may also be used, depending on the individual case. Treatment options for non-melanoma and melanoma will differ depending on where the cancer is, your general health and if it has spread.
The take-home message
The best protection against skin cancers involve a combination of sun safety measures and regular skin checks. That being said, while sunlight exposure brings potential risks, including skin damage and increased risk of skin cancer, it’s important to balance these negatives with the benefits sunlight can bring, such as: vitamin D synthesis, improved sleep, mood enhancement, and even better bone health.
If you’re interested in learning more about how to strike that balance and maximise the benefits of sunlight while minimising its negative effects, check out out articles on the benefits of natural light and vitamin D : why we need it and how to get more.
It is also important to regularly check your skin and be extra vigilant for any changes to moles, freckles and other skin lesions. Here are some tips on how to conduct a self-examination:
- Schedule regular skin checks: Set aside time every month to perform a thorough examination of your skin. This works best in a well-lit area with a full-length mirror.
- Examine your entire body: A handheld mirror may help with checking the hard to see areas, like your back or scalp. Alternatively, you may ask someone you trust to assist you and don’t forget to examine less obvious areas, such as the genital area and in between your toes.
- Look for changes in moles and lesions: This can be done using the ABCDE guide above.
- Check for new moles or lesions: Take note of any new growths on your skin that appear different to the surrounding skin.
- Monitor existing moles: Keep track of any changes in size, shape, colour or texture of moles you already have. You may find that taking pictures can be helpful to make future comparisons.
- Examine nails and nail beds: Inspect your fingernails and toenails, alongside the surrounding skin, for any unusual growths or changes.
- Seek professional evaluation: If you notice any suspicious changes, have concerns about your skin, or if you notice sores that don’t heal, consult with your GP.
Early detection is key for successful treatment of skin cancer. By incorporating regular self-examinations into our routine and promptly seeking guidance from a healthcare provider if we notice any changes, we can embrace a proactive approach to looking after our skin, prioritising wellbeing and self-care.
The Evergreen Life app has a built-in personal health record for you to store, update and track your health and wellness, helping you to gain a better picture of where your health is currently.
Reviewed by:
Anna Keeble MA BA Head of Content and Wellbeing Expert
Dr Claire Marie Thomas MRCGP DFSRH DTMH DipNLP MBChB BMedSci Medical Expert
- Bellenghi, M., Puglisi, R., Pontecorvi, G., De Feo, A., Carè, A. and Mattia, G. (2020). Sex and Gender Disparities in Melanoma. Cancers, [online] 12(7). Available here.
- Bendik, I., Friedel, A., Roos, F.F., Weber, P. and Eggersdorfer, M. (2014). Vitamin D: a critical and essential micronutrient for human health. Frontiers in Physiology, [online] 5. Available here.
- Boniol, M., Autier, P., Boyle, P. and Gandini, S. (2012). Cutaneous melanoma attributable to sunbed use: systematic review and meta-analysis. BMJ, 345(jul24 2), pp.e4757–e4757. Available here.
- Boutros, A., Cecchi, F., Tanda, E.T., Croce, E., Gili, R., Arecco, L., Spagnolo, F. and Queirolo, P. (2021). Immunotherapy for the Treatment of Cutaneous Squamous Cell Carcinoma. Frontiers in Oncology, 11. Available here.
- British Skin Foundation (n.d.). Are you at risk of skin cancer? [online] British Skin Foundation. Available here.
- British Skin Foundation (n.d.). Squamous cell carcinoma – British Skin Foundation. [online] http://knowyourskin.britishskinfoundation.org.uk . Available here.
- Buster, K.J., You, Z., Fouad, M. and Elmets, C. (2012). Skin cancer risk perceptions: A comparison across ethnicity, age, education, gender, and income. Journal of the American Academy of Dermatology, 66(5), pp.771–779. Available here.
- Cancer Research UK (2023). Soaring skin cancer cases hit a record high. [online] Cancer Research UK – Cancer News. Available here.
- Chalcraft, J.R., Cardinal, L.M., Wechsler, P.J., Hollis, B.W., Gerow, K.G., Alexander, B.M., Keith, J.F. and Larson-Meyer, D.E. (2020). Vitamin D Synthesis Following a Single Bout of Sun Exposure in Older and Younger Men and Women. Nutrients, 12(8), p.2237. Available here.
- Dennis, L.K., Vanbeek, M.J., Beane Freeman, L.E., Smith, B.J., Dawson, D.V. and Coughlin, J.A. (2008). Sunburns and Risk of Cutaneous Melanoma: Does Age Matter? A Comprehensive Meta-Analysis. Annals of Epidemiology, 18(8), pp.614–627. Available here.
- Heistein, J.B. and Acharya, U. (2023). Cancer, Malignant Melanoma. [online] PubMed. Available here.
- Kwiatkowska, M., Ahmed, S., Ardern‐Jones, M., Bhatti, L.A., Bleiker, T.O., Gavin, A., Hussain, S., Huws, D.W., Irvine, L., Langan, S.M., Millington, G.W.M., Mitchell, H., Murphy, R., Paley, L., Proby, C.M., Thomson, C.S., Thomas, R., Turner, C., Vernon, S. and Venables, Z.C. (2021). An updated report on the incidence and epidemiological trends of keratinocyte cancers in the United Kingdom 2013–2018. Skin Health and Disease, 1(4). Available here.
- Moan, J., Grigalavicius, M., Baturaite, Z., Dahlback, A. and Juzeniene, A. (2014). The relationship between UV exposure and incidence of skin cancer. Photodermatology, Photoimmunology & Photomedicine, 31(1), pp.26–35. Available here.
- Mullenders, L.H.F. (2018). Solar UV damage to cellular DNA: from mechanisms to biological effects. Photochemical & Photobiological Sciences, [online] 17(12), pp.1842–1852. Available here.
- Naik, P.P. and Farrukh, S.N. (2021). Influence of ethnicities and skin color variations in different populations- A Review. Skin Pharmacology and Physiology, 35(2). Available here.
- National Institute for Health and Care Excellence (2022a). Melanoma : What are the risk factors for melanoma? [online] NICE. Available here.
- National Institute for Health and Care Excellence (2022b). Melanoma: How common is melanoma? [online] NICE. [Accessed 9 Apr. 2024]. Available here.
- NHS (2017). Skin cancer (non-melanoma) – Treatment. [online] http://nhs.uk . Available here.
- NHS Choices (2019). Treatment – Skin cancer (melanoma). [online] NHS. Available here.
- NHS Inform (2023). Skin cancer (melanoma) symptoms and treatments. [online] www.nhsinform.scot. Available here.
- Oyebanjo, E. and Bushell, F. (2014). A critical evaluation of the UK SunSmart campaign and its relevance to Black and minority ethnic communities. Perspectives in Public Health, 134(3), pp.144–149. Available here.
- Seidl‐Philipp, M., Frischhut, N., Höllweger, N., Schmuth, M. and Nguyen, V.A. (2021). Known and new facts on basal cell carcinoma. Journal Der Deutschen Dermatologischen Gesellschaft, [online] 19(7), pp.1021–1041. Available here.
- Sinikumpu, S.-P., Jokelainen, J., Keinänen-Kiukaanniemi, S. and Huilaja, L. (2022). Skin cancers and their risk factors in older persons: a population-based study. BMC Geriatrics, 22(1). Available here.
- Skin Cancer Foundation (2022a). Basal Cell Carcinoma Warning Signs and Images. [online] The Skin Cancer Foundation. Available here.
- Skin Cancer Foundation (2022b). Squamous Cell Carcinoma Risk Factors. [online] The Skin Cancer Foundation. [Accessed 8 Apr. 2024]. Available here.



