
Optimising your diet for IBS relief
If you live with irritable bowel syndrome (IBS), you may already have noticed that food can influence how your digestive system feels. Some meals may seem to trigger bloating, abdominal pain, diarrhoea, or constipation, while other foods appear easier to tolerate. You might have been looking for a step-by-step IBS diet for some time.
It’s also therefore natural to wonder whether there is a specific “IBS diet” that can solve the problem.
Current research suggests the situation is more complex. IBS isn’t a single disease with a single cause. Instead, it’s thought to involve several interacting processes:
- including changes in how the gut moves,
- how sensitive the gut nerves are, and
- how the brain and digestive system communicate (known as the gut-brain axis).
The gut microbiome – the community of microorganisms, including bacteria, viruses and fungi, living in your digestive tract, mainly in your large intestine – may also play a role in IBS for some people.
Stop looking for the best diet for IBS and start figuring out the best diet for your IBS
Because these mechanisms vary from person to person, no single diet works for everyone with IBS. Instead, the most effective dietary approach usually involves a mix of general healthy eating principles, evidence-informed dietary strategies, and some degree of personal experimentation.
Clinical guidelines from organisations such as the National Institute for Health and Care Excellence (NICE) and the British Society of Gastroenterology recommend a stepwise approach to dietary management.Rather than immediately adopting a highly restrictive diet, most people benefit from starting with simple, structured eating habits and reviewing common triggers, such as caffeine, alcohol, meal timing, and fibre intake.
If symptoms continue despite these changes, more structured dietary strategies can then be considered. The best-studied of these approaches is the low-FODMAP diet, which reduces certain types of fermentable carbohydrates that can trigger symptoms in some people with IBS.
Fermentable carbohydrates are types of sugars and fibres that your body doesn’t fully digest or absorb in the small intestine. Instead, they travel to your large bowel (colon), where your gut bacteria break them down (ferment them).
They’re carbs that become food for your gut bacteria. When they’re fermented, the bacteria produce gas (like hydrogen and methane) and other substances that can affect how your gut works. For some people, especially those with sensitive guts, the gas and other substances produced can lead to bloating, wind, abdominal discomfort and changes in bowel habits.
Common examples include:
– certain fruits like apples and pears,
– some vegetables like onions and garlic,
– beans and lentils,
– dairy products (because of the lactose in them) and
– wheat products.
Not everyone reacts to these foods in the same way. Many people can tolerate them well and they can support a healthy gut.
Your gut bacteria can adapt over time. By slowly and regularly reintroducing certain foods, some people find their gut becomes better at handling them, with fewer symptoms. However, this doesn’t work for everyone and this article is designed to help you explore your gut and dietary needs at your own pace.
However, even structured dietary approaches don’t work for everyone. IBS is commonly divided into different symptom patterns – such as constipation-predominant IBS, diarrhoea-predominant IBS, where those are the main symptom, or mixed bowel habits – and these patterns may sometimes respond better to different dietary adjustments.
Researchers are also beginning to understand that people with IBS may have different gut microbiome patterns and metabolic responses to food. These differences may help explain why a dietary strategy that works well for one person may have little effect for another.
For these reasons, the goal of IBS dietary management is usually not to find a perfect universal diet, but rather to identify a pattern of eating that supports your digestive system, while still allowing you to enjoy a varied and sustainable diet.
In this article, we’ll look at:
- simple evidence-informed eating habits that help many people living with IBS
- dietary strategies that have been studied in clinical research
- how different IBS symptom patterns may respond to various approaches
- why people can respond differently to the same diet
The aim isn’t to recommend a restrictive set of rules, but to help you understand which dietary approaches are most likely to be worth trying, and how to test them in a practical and sustainable way.
Jump to section
- 1. Start with simple, structured eating habits
- 2. If symptoms continue, try evidence-informed dietary strategies
- 3. Adjust your diet based on your IBS pattern and personal response
Step-by-step IBS diet guide: Step 1. A simple starting point: General IBS eating principles
Before trying restrictive diets or avoiding large groups of foods, most clinical guidelines recommend starting with simple changes to eating habits and food patterns. For some people with IBS, these steps may meaningfully improve symptoms.
The digestive system is strongly influenced by how and when we eat. Large meals, irregular eating patterns, caffeine, alcohol, and certain types of fibre can all affect gut movement, fluid balance in the bowel, and gas production. When the digestive system is already sensitive – as it often is in IBS -these effects can become more noticeable.
For this reason, guidelines from organisations, such as NICE and the British Society of Gastroenterology, recommend beginning with structured eating habits and basic dietary adjustments before moving on to more restrictive approaches, if these are necessary.
Eat regular meals
Try to eat regular meals spaced evenly throughout the day.
Long gaps between meals followed by large meals can trigger stronger digestive reflexes. When food enters your stomach, your body activates what’s called the gastrocolic reflex – a normal, healthy signal that stimulates movement in your large intestine. In people with IBS, this reflex may be exaggerated, sometimes causing abdominal pain, urgency to have a bowel movement, or diarrhoea soon after eating.
Eating smaller, more regular meals can help keep these digestive signals steadier and reduce sudden bowel stimulation.
Practical tips include:
- Aim for three regular meals per day
- Avoid skipping meals
- Try not to leave long gaps between meals
- Consider smaller portions if large meals trigger symptoms
Avoid very large meals
Very large meals can stretch your stomach and trigger stronger gut contractions.
This can worsen symptoms, such as:
- abdominal pain
- bloating
- urgency
- diarrhoea
Some people find it helpful to divide large meals into smaller portions or include a light snack between meals instead.
Review your caffeine intake
Caffeine stimulates your digestive system and can increase bowel movement activity.
For people with IBS – particularly those with mainly diarrhoea symptoms – this can worsen urgency or loose stools.
Common sources of caffeine include:
- coffee
- tea
- energy drinks
- cola
- some sports drinks
NICE guidance suggests limiting caffeine intake to around three cups of tea or coffee per day, if symptoms are problematic.
Reducing caffeine gradually is often easier than stopping suddenly.
IBS bloating diet tips: Be cautious with fizzy drinks
Carbonated drinks contain dissolved gas. When this gas is released in your stomach and intestines, it can contribute to:
- bloating
- abdominal discomfort
- increased belching
Because people with IBS often have increased sensitivity to intestinal gas, fizzy drinks may make symptoms worse for some individuals.
Reducing intake of carbonated drinks can sometimes reduce bloating.
Limit alcohol if it worsens symptoms
Alcohol can affect digestion in several ways:
- increasing gut motility (movement)
- irritating the intestinal lining
- influencing gut bacteria and intestinal permeability (where the gut lining becomes more “leaky”, potentially allowing bacterial products to pass into the bloodstream and trigger inflammation).
These effects may contribute to symptoms, such as diarrhoea, abdominal pain, or reflux in some people.
Many people with IBS find symptoms are triggered mainly by larger amounts of alcohol, rather than occasional small amounts.
Understanding fibre: not all fibre behaves the same way
Fibre is often recommended for digestive health, but in IBS the type of fibre matters.
Two main types of fibre behave differently in your digestive system.
Soluble fibre
Soluble fibre dissolves in water and forms a soft gel-like substance your the bowel. This can help regulate stool consistency and support smoother bowel movements.
Examples of soluble fibre include:
- oats
- psyllium husk
- linseeds (flaxseed)
- chia seeds
- some fruits and vegetables, including ripe bananas, apples and pears (without skins), carrots, parsnips, chickpeas, cooked broccoli and cauliflower, avocado etc.
Research suggests soluble fibre can improve overall IBS symptoms, particularly when constipation is a main symptom.
Insoluble fibre
Insoluble fibre adds bulk to stool and can stimulate bowel movement more aggressively.
Examples of insoluble fibre include:
- wheat bran
- whole wheat products
- some cereals, for instance Weetabix, Shredded Wheat, Bran Flakes
- nuts, seeds peanut butter
While insoluble fibre can help some people with constipation, it may worsen symptoms, such as bloating, gas, and abdominal pain in many people with IBS.
For this reason, guidelines often recommend favouring soluble fibre over bran-based fibre.
Introduce fibre gradually
Increasing fibre too quickly can lead to:
- gas
- bloating
- abdominal discomfort
If you increase fibre intake, it’s usually best to do so slowly over several weeks, allowing your digestive system time to adapt.
Drinking enough non-caffeinated fluids like water or herbal tea, is also important when increasing fibre intake.
For more information on how to balance fibre with fluids, head over to our Hydration and IBS: Tips on fluid intake for digestive health article.
Identify your personal food triggers
Many people living with IBS notice that certain foods trigger symptoms. Common examples include:
- spicy foods
- fatty meals
- onions or garlic
- some dairy products
- artificial sweeteners
However, triggers vary widely between individuals.
Keeping a simple symptom and food diary for a few weeks can sometimes reveal patterns and help guide dietary adjustments.
Why these simple steps often help
These basic strategies address several common factors involved in IBS symptoms, including:
- digestive reflexes triggered by meals
- bowel movement patterns
- intestinal gas production
- gut sensitivity
For some people, these adjustments alone can significantly improve symptoms.
If symptoms continue despite these changes, more structured dietary strategies – such as the low-FODMAP diet – may then be worth exploring.
Step-by-step IBS diet guide: Step 2. Evidence-informed dietary strategies: The low-FODMAP diet for IBS
If basic eating habits and fibre adjustments don’t fully improve IBS symptoms, a more structured dietary approach may sometimes help.
The most widely studied dietary strategy for IBS is the low-FODMAP diet. Clinical trials and systematic reviews suggest that reducing certain fermentable carbohydrates can improve symptoms, such as abdominal pain, bloating, and changes in bowel habit in many people with IBS.
A systematic review is a structured review and analysis of all available high quality evidence and literature on a certain topic. The way they’re carried out tends to minimise bias and ensure results can be reproduced.
However, like most IBS treatments, it doesn’t work for everyone. The low-FODMAP diet is best understood as a method for identifying dietary triggers, rather than a permanent restrictive diet.
What are FODMAPs?
FODMAP stands for Fermentable Oligosaccharides, Disaccharides, Monosaccharides and Polyols.
These carbohydrates are sometimes poorly absorbed in the small intestine. When they pass into the large intestine they can affect digestion in two main ways:
- they draw water into the bowel, which may contribute to loose stools or diarrhoea,
- they’re rapidly fermented (broken down) by gut bacteria, producing gas.
This combination of increased fluid and gas can stretch the bowel. Because people with IBS often have heightened sensitivity to intestinal stretching, this may trigger symptoms, such as bloating, abdominal pain, and urgency.
Foods that contain FODMAPs
FODMAP carbohydrates appear naturally in many foods.
Examples include:
Oligosaccharides:
- wheat
- rye
- onions
- garlic
- legumes
Disaccharides:
- lactose in milk and soft cheeses
Monosaccharides:
- excess fructose in fruits, such as apples and mango
Polyols:
- sweeteners such as sorbitol or mannitol
- fruits, such as plums and peaches
Many of these foods are nutritious and part of a healthy diet. So, the aim of a low-FODMAP approach isn’t to eliminate them permanently from your diet, but to identify which ones may trigger symptoms.
Evidence for the low-FODMAP diet for IBS
The low-FODMAP diet was originally developed by researchers at Monash University and has now been studied in many clinical trials.
A landmark randomised controlled trial (RCT) showed that reducing FODMAP intake significantly improved IBS symptoms compared with a typical control diet.
Participants in RCT studies are randomly assigned to different treatments to limit bias. They’re considered one of the most reliable study designs.
In research studies, a “control intervention” is a specific, planned treatment, procedure or condition experienced by the group of study participants known as the “control group”. It’s used to provide a baseline for comparison against the experimental intervention. In the RCT above, an Australian diet was used as the control intervention/diet to give the researchers something to compare the experimental interventions, in this case, a low-FODMAP diet, to.
More recent systematic reviews and network meta-analyses have confirmed that low-FODMAP diets can improve overall IBS symptom scores and reduce symptoms, such as abdominal pain and bloating.
A meta-analysis is a statistical technique that combines and analyses data from multiple independent studies in an attempt to answer the same research question to reach a more precise, overarching conclusion. It increases sample size and power, overcoming contradictions among individual studies.
Meta-analyses are often thought of as the highest level of evidence, particularly in medical research.
For this reason, major gastroenterology guidelines consider the low-FODMAP diet to be one of the most evidence-supported dietary strategies for IBS, particularly when initial lifestyle and dietary advice hasn’t worked.
Why the low-FODMAP diet works for some people
Researchers believe the low-FODMAP diet works mainly by reducing intestinal gas production and fluid shifts in the bowel.
People with IBS often experience:
- increased sensitivity of their gut nerves,
- altered movement of their bowel,
- stronger responses to gas and intestinal stretching.
By reducing highly fermentable carbohydrates, the low-FODMAP diet may limit the triggers that provoke these responses in some individuals.
The three phases of the low-FODMAP diet plan
Clinical guidelines emphasise that the low-FODMAP diet should be followed in three phases, rather than as a long-term elimination diet.
1. Restriction phase
For a short period (usually 2–6 weeks), foods high in FODMAPs are reduced.
This helps determine whether these carbohydrates may be contributing to symptoms.
2. Reintroduction phase
Foods are then gradually reintroduced, usually one FODMAP group at a time.
This allows people to identify which specific carbohydrates trigger symptoms.
Many people discover that they’re sensitive to only one or two FODMAP groups, rather than all of them.
3. Personalisation phase
The long-term goal is a personalised diet including as many tolerated foods as possible.
This helps maintain nutritional balance and supports a healthy gut microbiome.
Effects on the gut microbiome
Some studies have found that strict low-FODMAP diets may reduce levels of beneficial gut bacteria, such as Bifidobacteria, because fermentable carbohydrates also act as food for these microbes. As yet, we don’t know how long this impact lasts. One small study did find evidence that gradual FODMAP reintroduction and personalisation following a short-term low-FODMAP restrictive diet may normalise some of the effects of short-term restriction on the gut microbiome, whilst maintaining improved symptoms. However, there isn’t enough evidence currently to fully understand the long term impact.
For this reason, most experts recommend reintroducing tolerated foods after the initial restriction phase, rather than maintaining a strict low-FODMAP diet indefinitely.
At the time of writing, emerging research also suggests that people with IBS may have different microbiome patterns, which could partly explain why some individuals respond better to dietary changes than others.
Who might benefit most from trying a low-FODMAP diet?
Research suggests the diet may be particularly helpful for people with IBS who experience:
- significant bloating,
- abdominal pain after eating,
- excessive gas,
- diarrhoea or mixed bowel patterns.
However, it may be less helpful when constipation is the dominant symptom, unless bloating and pain are also prominent.
When to seek dietary guidance
Because the low-FODMAP diet can be restrictive, many guidelines recommend trying it with the support of a dietitian where possible.
Professional guidance can help ensure that:
- the diet remains nutritionally balanced,
- unnecessary foods aren’t excluded,
- tolerated foods are reintroduced appropriately.
A balanced approach
Although the low-FODMAP diet currently has the strongest evidence among IBS dietary strategies, it isn’t always the first step.
For many people, symptoms improve with the simpler measures discussed above, such as:
- regular meal patterns,
- moderating caffeine and alcohol intake,
- adjusting fibre intake.
The low-FODMAP diet is best viewed as one tool within a broader strategy to understand your individual digestive triggers.
Step-by-step IBS diet guide: Step 3. Adjust your diet based on your IBS pattern and personal response
Different IBS patterns may respond to different dietary approaches
IBS is usually divided into subtypes based on stool pattern, which can help guide treatment approaches. These patterns are defined using stool consistency and frequency and include:
- IBS-C – constipation-predominant
- IBS-D – diarrhoea-predominant
- IBS-M – mixed bowel habits (alternating constipation and diarrhoea)
These patterns reflect differences in how the digestive system behaves. For example, some people may experience slower bowel movements and harder stools, while others have faster transit and looser stools.
Researchers believe that a combination of factors may contribute to these differences, including:
- gut motility (how quickly food moves through the digestive tract)
- gut sensitivity (known as visceral hypersensitivity)
- interactions between the gut and nervous system
- gut microbial activity
- the way the bowel handles water and bile acids.
Because of these differences, dietary strategies may sometimes work better for one IBS pattern than another.
However, the scientific evidence for subtype-specific diets is still evolving. Most dietary strategies are therefore best approached through careful trial and observation, rather than strict rules.
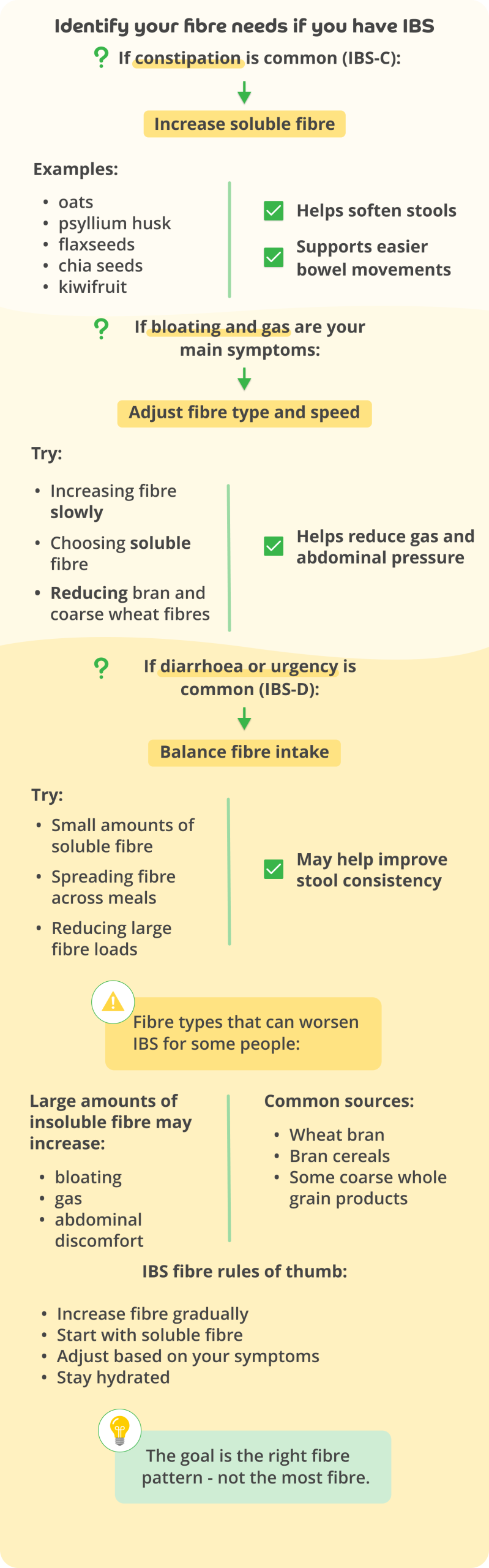
IBS-C: Constipation-predominant IBS
In IBS-C, the bowel tends to move more slowly, leading to symptoms, such as:
- infrequent bowel movements,
- hard or difficult-to-pass stools,
- abdominal discomfort or bloating.
For this pattern, eating soluble fibre may be a helpful dietary strategy.
Soluble fibre (see above) absorbs water and forms a soft gel in the digestive tract. This can help increase stool moisture and make bowel movements easier to pass. Research has shown that soluble fibre like psyllium can improve overall IBS symptoms, particularly when constipation is present.
In contrast, insoluble fibre, such as wheat bran, may worsen symptoms for some people with IBS by increasing gas and abdominal discomfort.
For people with IBS-C who also experience significant bloating or abdominal pain, a low-FODMAP diet may still be helpful. However, because the diet reduces certain fermentable carbohydrates that can support gut bacteria, it’s generally used carefully and followed by gradual reintroduction of tolerated foods.
IBS-D: Diarrhoea-predominant IBS
In IBS-D, bowel movements tend to happen more often and may be loose or urgent. Common symptoms include:
- loose stools,
- urgency,
- abdominal pain after meals,
- bloating or gas.
The low-FODMAP diet often appears particularly helpful for this pattern. By reducing poorly absorbed carbohydrates that draw water into the bowel and ferment rapidly, the diet may help reduce diarrhoea and bloating (due to the production of gas from fermentation).
Some people with IBS-D also notice that symptoms are triggered and/or worsened by high-fat meals, possibly by affecting gut movement and sensitivity.
Interestingly, researchers have found that a proportion of people with chronic diarrhoea may have bile acid-related mechanisms, where bile acids reach the large intestine (colon) and stimulate fluid secretion (production and discharge) and bowel activity. In addition, there’s evidence that bile-acid diarrhoea is misdiagnosed in up to 30% of diarrhoea-predominant patients with IBS.
Although this doesn’t apply to everyone with IBS-D, it may partly explain why certain foods trigger symptoms in some individuals.
IBS-M: Mixed bowel pattern IBS
People with IBS-M experience alternating patterns of constipation and diarrhoea.
Because symptoms vary, dietary management can be more complex. Strategies often focus on:
- maintaining regular meal patterns,
- adjusting fibre intake carefully,
- identifying individual trigger foods.
In some cases, a low-FODMAP diet may help reduce symptoms, such as bloating and abdominal pain, even if bowel habits vary.
However, because bowel patterns can change over time, dietary strategies often need to be flexible and personalised.
Why individual responses vary
One of the challenges of managing IBS through diet is that people respond differently to the same foods.
Several factors may influence this variation, including:
- differences in the make-up of the gut microbiome,
- variation in gut sensitivity,
- differences in digestive enzyme activity (digestive enzymes are specialised proteins produced by your body (mainly by your pancreas, stomach, and small intestine) that break down food into small, absorbable nutrients like simple sugars, amino acids, and fatty acids),
- how quickly food moves through the digestive tract.
Recent research has suggested that some IBS patients may have different gut microbiome patterns, which may influence how they respond to diets, such as the low-FODMAP diet.
However, this area of research is still developing, and, at the time of writing, routine microbiome testing isn’t currently recommended for guiding dietary treatment.
A practical approach
Because IBS varies widely between individuals, dietary management usually works best when it follows a stepwise and personalised approach:
- Start with basic dietary and lifestyle adjustments.
- Adjust fibre intake depending on symptoms.
- Consider structured approaches, such as a low-FODMAP diet, if symptoms continue.
- Reintroduce foods and identify personal triggers.
Over time, this approach helps many people find a sustainable way of eating that supports digestive comfort without unnecessary restriction.
Why do people respond to different diets?
One of the most common questions people ask about IBS diets is: “Why does a food trigger symptoms for one person but not another?”
Researchers believe several biological factors may explain why dietary responses vary between individuals with IBS.
- differences in gut sensitivity,
- variation in gut movement patterns (motility),
- differences in the gut microbiome,
- how carbohydrates are fermented by gut bacteria,
- variation in bile acid metabolism.
Because IBS involves a complex interaction between the digestive system, nervous system and gut microbes, it’s unlikely that a single diet will work for everyone.
Instead, dietary strategies often work best when they are tested and adapted based on individual responses.
Gut sensitivity
Many people with IBS experience visceral hypersensitivity, meaning the nerves in their digestive tract respond more strongly to normal stretching of the bowel.
This means that amounts of gas or fluid that might not cause symptoms in other people may trigger:
- abdominal pain,
- bloating,
- discomfort.
Reducing foods that increase gas production – such as highly fermentable carbohydrates – may therefore minimise symptoms for some individuals.
Gut movement patterns
The speed at which food moves through the digestive tract can vary between people with IBS.
Some individuals experience slower intestinal transit, which can contribute to constipation and bloating. Others experience faster bowel movement, which may lead to diarrhoea and urgency.
These differences can influence how the digestive system responds to particular foods or dietary patterns.
Fermentation of carbohydrates
Many carbohydrates reach the large intestine where they’re fermented (broken down) by gut bacteria.
During fermentation, bacteria produce gases, such as hydrogen and methane. In people with IBS who have increased gut sensitivity, this gas production may contribute to symptoms including:
- bloating,
- abdominal discomfort.
Reducing certain fermentable carbohydrates – as is seen in the low-FODMAP diet – can therefore improve symptoms for some individuals.
The gut microbiome
The gut microbiome refers to the community of bacteria and other microorganisms living in the digestive tract.
These microbes help break down food, produce metabolites, and interact with the immune and nervous systems.
Studies suggest that people living with IBS may have different microbiome compositions (make up) and metabolic activity compared with people without IBS.
Some research has also identified distinct microbiome subtypes within IBS, which may partly explain why some people respond better to dietary changes like the low-FODMAP diet.
However, this area of research is still developing.
Bile acid metabolism
In some people, digestive symptoms may be influenced by the way the body processes bile acids, which are produced by the liver to help digest fats.
If excess bile acids reach the large intestine, they can stimulate fluid secretion and increase bowel activity. This may contribute to symptoms, such as:
- diarrhoea,
- urgency,
- abdominal discomfort.
Some studies suggest that bile acid-related mechanisms may contribute to symptoms in a proportion of people diagnosed with IBS-D.
Important caution: microbiome testing
Although microbiome research is expanding rapidly, routine microbiome testing isn’t currently recommended for guiding IBS treatment and isn’t available on the NHS at the time of publishing.
Current clinical guidelines emphasise that these tests are still experimental and don’t yet provide reliable information for individual dietary decisions.
As research develops, this may change in the future.
What this means in practice
Taken together, these findings help explain why dietary strategies for IBS often involve careful personal experimentation.
Two people with similar symptoms may respond very differently to the same diet because their digestive systems function differently.
For many people, the most effective approach involves:
- starting with general IBS dietary principles
- trying evidence-informed strategies, such as fibre adjustment or low-FODMAP diets
- gradually identifying individual food triggers over time.
This personalised approach allows people to find a sustainable way of eating that supports digestive comfort without unnecessary restriction.
Common IBS diet mistakes to avoid
Trying to improve IBS symptoms through diet can sometimes lead to overly restrictive eating patterns. While dietary changes can be helpful, removing too many foods too quickly can make eating unnecessarily difficult and may even reduce dietary variety and nutritional balance.
As discussed above, clinical guidelines generally recommend starting with simple dietary adjustments before moving to more restrictive strategies.
Common mistakes people make when trying to manage IBS through diet include:
Staying on strict elimination diets long term
Diets, such as the low-FODMAP diet, are designed to be used in stages. The initial restriction phase is usually followed by a structured reintroduction phase to identify which foods actually trigger symptoms.
Remaining on the strict elimination phase long term may reduce dietary diversity and can alter the gut microbiome.
Removing too many foods at once
Some people try eliminating multiple food groups simultaneously. While this may temporarily reduce symptoms, it can make it difficult to identify which foods are truly responsible.
A structured and gradual approach is usually more effective.
Assuming gluten is the main cause
Many people with IBS suspect gluten may be responsible for symptoms. However, research suggests that, in many cases, symptoms may be triggered instead by fermentable carbohydrates (FODMAPs) present in wheat and related foods.
For this reason, single food avoidance and structured dietary approaches, such as low-FODMAP diets, are generally recommended before adopting a strict gluten-free diet, unless coeliac disease has been diagnosed. (NICE recommends clinicians carry out antibody testing for coeliac disease in people who meet the IBS diagnostic criteria, to exclude other diagnoses).
Increasing bran or insoluble fibre
Fibre is often recommended for digestive health, but insoluble fibre, such as wheat bran can worsen symptoms in some people with IBS by increasing gas production and abdominal discomfort.
In contrast, soluble fibre tends to be better tolerated and has stronger evidence for improving IBS symptoms.
Relying on “gut detox” diets
Various diets often promoted online claim to “reset” or “detox” the gut microbiome.
At the time of writing, there is little scientific evidence supporting extreme detox approaches for IBS. Clinical guidelines emphasise structured, evidence-informed dietary strategies instead.
The goal of dietary management
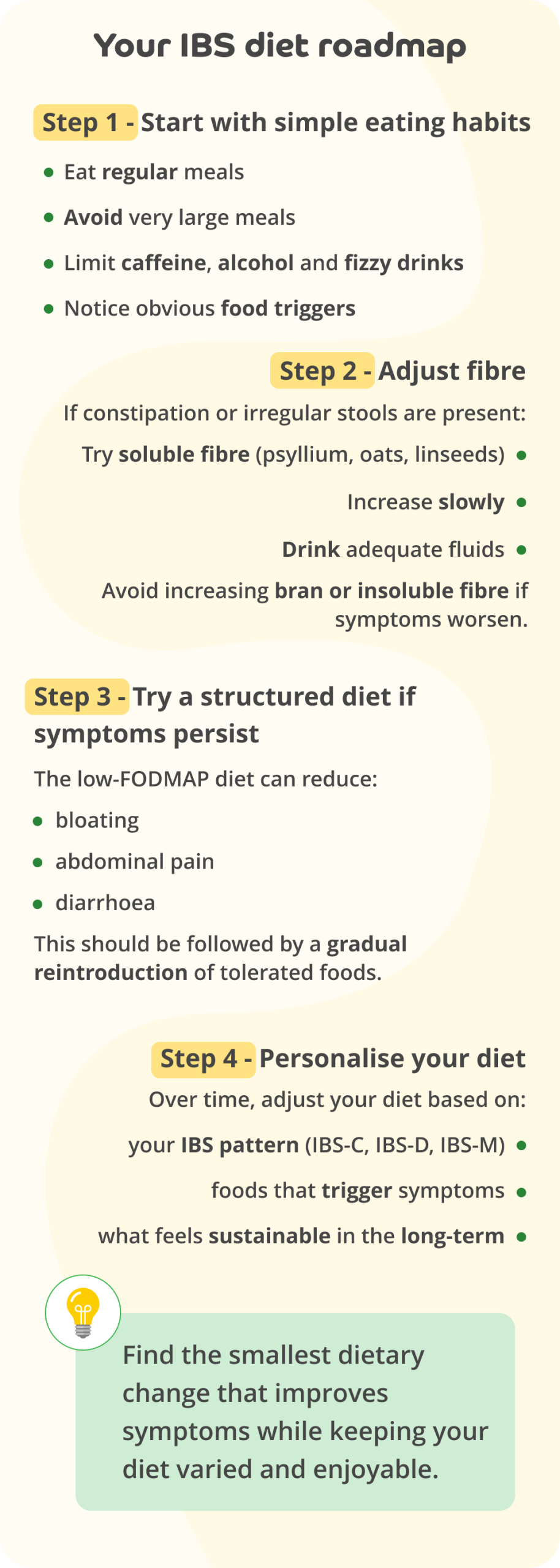
The aim of IBS dietary management isn’t to eliminate as many foods as possible, but rather to identify the smallest dietary change that improves symptoms, while maintaining a varied and sustainable diet.
A practical step-by-step IBS diet guide
Because IBS varies widely between individuals, many guidelines recommend a stepwise approach to dietary management.
This allows people to try simple strategies first before moving to more structured dietary interventions.
Step 1: Start with structured eating habits
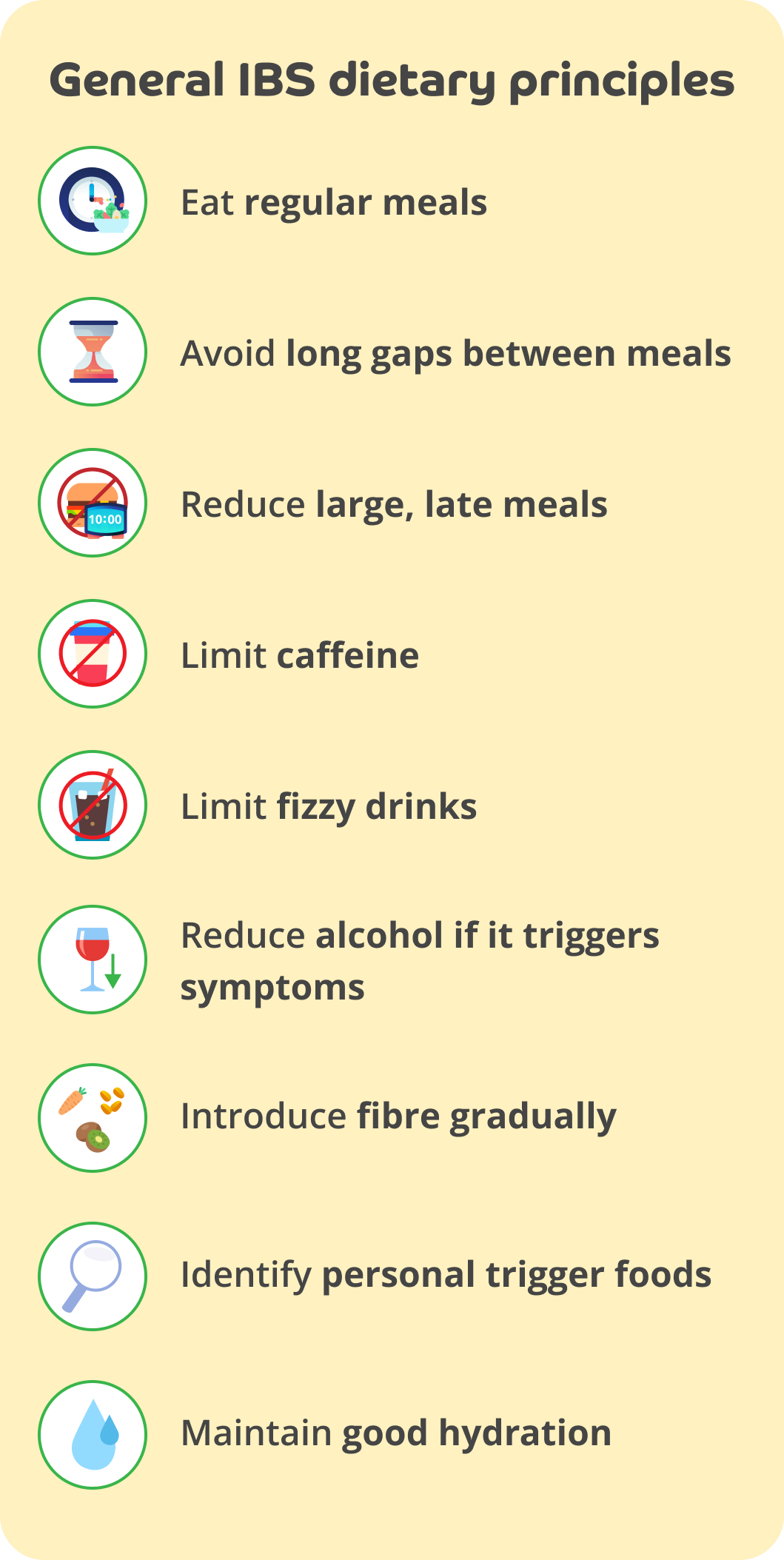
Begin with general IBS dietary principles, such as:
- eating regular meals
- avoiding very large meals
- reviewing caffeine and alcohol intake
- moderating carbonated, fizzy drinks
- identifying obvious personal food triggers.
For many people, these simple changes can significantly improve symptoms.
Step 2: Trial soluble fibre
If you often experience constipation or irregular bowel movements, increasing soluble fibre may help.
Examples include:
- psyllium husk,
- oats,
- linseeds (flaxseed).
Soluble fibre can improve stool consistency and overall IBS symptoms in some people.
Step 3: Consider a low-FODMAP diet
If symptoms continue despite making basic dietary adjustments, a low-FODMAP diet may be considered.
Research shows that reducing fermentable carbohydrates can improve symptoms, such as:
- bloating,
- abdominal pain,
- diarrhoea.
Because the diet is restrictive, it’s usually followed by gradual reintroduction of tolerated foods (and wise to do it with the support of a registered dietician).
Step 4: Personalise your diet
Over time, dietary strategies can be adjusted based on:
- your IBS subtype (constipation-predominant, diarrhoea-predominant, or mixed,
- your individual food responses,
- your symptom patterns.
This personalised approach helps people develop a sustainable long-term eating pattern rather than relying on highly restrictive diets.
How to manage IBS through diet: Key takeaways
- There’s no single IBS diet that works for everyone.
- Start with simple structured eating habits before trying restrictive diets.
- Soluble fibre and low-FODMAP diets have the strongest evidence for improving symptoms.
- Different IBS patterns may respond better to different dietary approaches.
- Although there’s no doubt that IBS is challenging to live with, patience to achieve personalisation and try gradual testing is needed as they’re usually the most effective long-term strategies.
Professional support for IBS diets
If you’d like more support managing IBS symptoms, the following resources may be helpful:
- NHS IBS information
- The Guts UK Charity (UK patient charity)
- British Dietetic Association IBS resources
A registered dietitian can help guide structured approaches, such as the low-FODMAP diet and support safe food reintroduction.
This article provides general educational information about diet and irritable bowel syndrome (IBS). It is not intended to diagnose medical conditions or replace personalised advice from a healthcare professional.
Dietary responses vary widely between individuals. If you are considering major dietary changes, or if your symptoms are severe or persistent, it is advisable to discuss this with your GP or a registered dietitian.
People with coeliac disease, inflammatory bowel disease, or other digestive conditions may require different dietary management.
Seek medical advice if you experience any of the following symptoms, as these are not typical features of IBS and may require medical assessment:
– unexplained weight loss
– blood in your stool
– persistent diarrhoea, especially at night
– unexplained anaemia
– severe or worsening abdominal pain
– symptoms beginning after age 50
If your symptoms change suddenly or significantly worsen, you should also speak to a healthcare professional
- Bijkerk CJ, de Wit NJ, Muris JW, Whorwell PJ, et al. Soluble or insoluble fibre in irritable bowel syndrome in primary care? Randomised placebo controlled trial. BMJ. 2009 Aug 27; 339: b3154. doi: 10.1136/bmj.b3154.
- Bishehsari F, Magno E, Swanson G, et al. Alcohol and Gut-Derived Inflammation. Alcohol Res. 2017; 38(2): 163-171. doi: 10.35946/arcr.v38.2.02.
- Black CJ and Ford AC. Global burden of irritable bowel syndrome: trends, predictions and risk factors. Nat Rev Gastroenterol Hepatol. 2020 Aug; 17(8): 473-486. doi: 10.1038/s41575-020-0286-8.
- Boekema P, Samsom M, van Berge Henegouwen GP, et al. Coffee and Gastrointestinal Function: Facts and Fiction: A Review. Scandinavian Journal of Gastroenterology. 1999 Feb; 230(34): 35-9. doi: 10.1080/003655299750025525.
- British Dietetic Association (n.d.) Irritable bowel syndrome (IBS) and diet. [Accessed 17/03/2026].
- Camilleri M. Bile Acid diarrhea: prevalence, pathogenesis, and therapy. Gut and Liver. 2015 May 23; 9(3): 332-9. doi: 10.5009/gnl14397.
- Chey WD, Hashash JG, Manning L, et al. AGA Clinical Practice Update on the Role of Diet in Irritable Bowel Syndrome: Expert Review. Gastroenterology. 2022 May; 162(6): 1737-1745.e5. doi: 10.1053/j.gastro.2021.12.248.
- Cuffe MS, Staudacher HM, Aziz I, et al. Efficacy of dietary interventions in irritable bowel syndrome: a systematic review and network meta-analysis. The Lancet Gastroenterology & Hepatology. 2025 Jun; 10(6): 520-536. doi: 10.1016/S2468-1253(25)00054-8.
- Farrugia A and Arasaradnam RP. Bile acid diarrhoea: pathophysiology, diagnosis and management. Frontline Gastroenterology. 2020 Sept; 12: 500-507. doi: 10.1136/flgastro-2020-101436.
- Feinle-Bisset C and Azpiroz F. Dietary lipids and functional gastrointestinal disorders. Am J Gastroenterol. 2013 May; 108(5): 737-47. doi: 10.1038/ajg.2013.76.
- Ford AC, Lacy BE, Talley NJ. Irritable bowel syndrome. New England Journal of Medicine. 2017.
- Guts UK (n.d.) It’s time to get to grips with guts. [Accessed 17/03/2026].
- Halmos EP, Power VA, Shepherd SJ, et al. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology. 2014 Jan; 146(1): 67-75.e5. doi: 10.1053/j.gastro.2013.09.046.
- Lacy BE, Pimentel M, Brenner DM, et al. ACG Clinical Guideline: Management of Irritable Bowel Syndrome. The American Journal of Gastroenterology. 2021 Jan; 116(1): 17-44. doi: 10.14309/ajg.0000000000001036.
- Malone JC and Thavamani A. Physiology, Gastrocolic Reflex. Treasure Island (FL) StatPearls Publishing. 2023 May.
- Monash University (n.d.) Discover the research Behind the Low FODMAP Diet. [Accessed 17/03/2026].
- NHS (n.d.) Irritable bowel syndrome (IBS). [Accessed 17/03/2026].
- NICE (2017) Irritable bowel syndrome in adults: diagnosis and management. Recommendations.
- Staudacher HM, Lomer MCE, Anderson JL, et al. Fermentable Carbohydrate Restriction Reduces Luminal Bifidobacteria and Gastrointestinal Symptoms in Patients with Irritable Bowel Syndrome. Journal of Nutrition. 2012 Aug; 142(8): 1580-1518. doi: 10.3945/jn.112.159285.
- Pittayanon R, Lau JT, Yuan Y, et al. Gut Microbiota in Patients With Irritable Bowel Syndrome-A Systematic Review. Gastroenterology. 2019 Jul; 157(1): 97-108. doi: 10.1053/j.gastro.2019.03.049.
- Staudacher HM and Whelan K. The low FODMAP diet: recent advances in understanding its mechanisms and efficacy in IBS. Gut. 2017 Aug; 66(8): 1517-1527. doi: 10.1136/gutjnl-2017-313750.
- Staudacher HM, Rossi M, Kaminski T, et al. Long-term personalized low FODMAP diet improves symptoms and maintains luminal Bifidobacteria abundance in irritable bowel syndrome. Neurogastroenterol Motil. 2022 Apr; 34(4): e14241. doi: 10.1111/nmo.14241.
- Vasant DH, Paine PA, Black CJ, et al. British Society of Gastroenterology guidelines on the management of irritable bowel syndrome. Gut. 2021 Apr; 0:1-27. doi: 10.1136/gutjnl-2021-324598.
- Vervier K, Moss S, Kumar N, et al. Two microbiota subtypes identified in irritable bowel syndrome with distinct responses to the low FODMAP diet. Gut. 2022 Sep; 71(9): 1821-1830. doi: 10.1136/gutjnl-2021-325177.
- West Suffolk NHS Foundation Trust (n.d.) Fibre. [Accessed 17/03/2026].



