
It’s amazing when you think about how we can get embarrassed about the subject of an organ half the population has between their legs and how those with said organ perform with it, but embarrassed we get. Talking about penis health, such as erectile dysfunction, isn’t just important for breaking the taboo, it’s also vital as it can be an indicator of other, preventable, health issues, as we’ll explore in this article.
What is erectile dysfunction?
Erectile dysfunction (ED), otherwise known as impotence, is where a male either struggles to get an erection or has difficulty keeping one long enough to have penetrative sex. It can be more common than you think, especially in men aged over 40. In fact, it’s thought that half of all men between the ages of 40 and 70 will experience it to some extent.
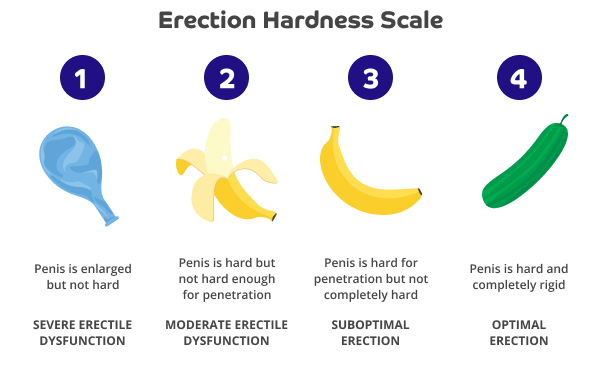
What do we mean ‘by some extent’? It can be tricky to articulate subjective perceptions of experiences, particularly around perceived “taboo” subjects, like erectile dysfunction, so it can be easier to refer to objective numbers. To this end, an Erection Hardness Score (EHS) was devised in 1998, used by some clinicians:
What does good penile health look like?
Whilst morning erections or “Morning glory” are normal, they aren’t an essential sign of penile health. This is because testosterone naturally declines after the age of 40, meaning a possible lack of morning erections for older men. Another important factor is that erections are usually fleeting, lasting only a few minutes so you may not know you’ve had one. That being said, the absence of erections may be an indicator of other possible issues besides ED, such as testosterone deficiency, structural issues or atherosclerosis (see below). An erection that lasts too long is also a cause for concern.
There may be some associations between symptoms and mortality. For instance, in a study of 1,788 men aged 40-79, men with ED, reduced morning erections and lower libido (sex drive) had a higher mortality risk compared to men without these symptoms. ED, in particular, predicted all-cause mortality and potentially serves as a warning sign of poor health status in older men. However, despite these associations, it doesn’t necessarily mean erectile dysfunction causes high mortality rates, and not having “morning wood” every day isn’t a concrete sign of problems.
The key message is to consult your GP if you feel something is wrong as they can work with you on a personal level and rule out other scenarios.They’re likely to ask you about your ability to get and maintain an erection and to have penetrative sex (or, if you’re not having sex, they’ll enquire about any masturbation symptoms you have, your ability to climax, if you have any pain when you do, or any urinary symptoms, swellings or lumps. These types of questions are often asked in urology (a branch of medicine that focuses on disorders in the urinary system) to assess the seriousness of ED and monitor treatment.
If you have erectile dysfunction can you still get hard?
Yes, depending on the cause, you may still get an erection at other times unrelated to sex, such as when you wake up. As we’ll see later, erectile dysfunction can be preventable and reversible with some lifestyle changes.
Why is monitoring signs of erectile dysfunction so important?
With ED being suggested as being a marker of cardiovascular diseases, penis problems could very well be a sign that those experiencing them could be at risk of a cardiac event. After all, when the arteries in the heart get clogged it can often result in a heart attack. With the arteries to the penis being a lot smaller at 1mm in diameter, compared to the heart’s 3mm artery diameter, those penis arteries are likely to develop plaque and clog long before the heart arteries.
Additionally, men experiencing diabetes are three times more likely to have ED due to, among other things, limited blood flow, blood vessel damage and impaired nerves (neuropathy). So, problems with erections could also, although not always, be a sign of developing diabetes. Type 2 diabetes can be prevented if certain lifestyle changes are made.
Among men in our Evergreen Life community, high HbA1c (your average blood glucose (sugar) levels for the last two to three months), is significantly associated with an unsatisfying sex life. Type 2 diabetes is a condition that causes the level of sugar in the blood to become too high.
Erectile dysfunction and heart disease: what does the research say?
Cardiovascular diseases is a general term referring to conditions impacting the heart or blood vessels. A meta-analysis of 12 prospective cohort studies involving 36,744 people found strong evidence that ED is significantly and independently associated with an increased risk of not only cardiovascular diseases, but coronary heart disease, stroke and all-cause mortality too. What’s more, a more recent meta analysis of 25 studies featuring 154,794 people, concluded that the risk of total cardiovascular disease, coronary heart disease, stroke, and all-cause mortality was significantly increased in populations with ED, and that severe ED is of particular concern.
Added to this, lower total serum testosterone levels were associated with erectile dysfunction in a study involving 802 male intermediate cardiovascular risk patients, according to the Framingham Risk Score (a simplified and common tool used to determine cardiovascular disease risk level over 10 years). Lower testosterone levels were also associated with impaired flow-mediated vasodilation. When flow mediated vasodilation occurs in large arteries it’s an established marker for early atherosclerosis – where your arteries become narrowed, making it harder for blood to travel through them, increasing your risk of heart attack and stroke.
These associations are significant because other studies have shown lower testosterone levels are associated with chronic medical conditions, for example, metabolic syndrome, type 2 diabetes, dyslipidemia, hypertension – all of which are cardiovascular disease risk factors – as well as being linked with cardiovascular (CV) events themselves.
What causes erectile dysfunction?
Age is an influencing factor in the development of ED, with it mainly impacting men over 40. Yet, often there can be multiple, interconnected, modifiable, causes of erectile dysfunction:
Psychological causes:- Anxiety
- Depression
- Relationship issues
- Fears regarding sexual orientation
As ED and penis health are often shrouded in taboo, if spoken about at all, causes can often be psychogenic, that is, have a psychological origin rather than a physical one. For example, it’s not uncommon for middle-aged men to experience pro-longed perceived stress, a risk factor for ED. The stress they’re going through may spark a loss of skeletal muscle mass, which affects testosterone. Despite most men experiencing lower testosterone levels as they age, these levels aren’t usually low enough to induce ED, but people living with low testosterone levels often experience other chronic medical conditions, such as heart disease, high blood pressure and diabetes that can contribute to ED (see below).
There are nearly always psychological consequences of ED, relating to marital and relationship issues, cultural norms and expectations, loss of self-esteem, shame, anxiety, and depression, among others. ED can lead to significant emotional damage for a person and his partner, and have a considerable affect on their quality of life. Thus, the stress can contribute to the onset of ED, with the experience of sexual dysfunction causing more emotional distress, triggering a vicious cycle.
Organic causes (where there’s a measurable change to tissues, organs, or body systems):- Hypertension and cardiovascular diseases (particularly in older men)
- Diabetes mellitus and metabolic syndrome can impact many organ systems leading to quicker ED decline and can, at a molecular level, disturb the mechanisms supporting erections
- Physical trauma, such as pelvic fractures or spinal cord injuries
- Hyperlipidemia, a disorder that’s one of the most common risk factors contributing to the development of atherosclerosis, another ED cause
- Stroke
- Sleep apnoea
- COPD (Chronic Obstructive Pulmonary Disease)
- Glaucoma
- Sequela of priapism (where the penis remains long and rigid despite the lack of suitable stimulation as a result of a previous disease or injury)
- Prostatic hyperplasia (enlarged prostate) with lower urinary symptoms (benign prostatic hyperplasia with lower urinary tract symptoms)
- Iatrogenic (caused by medical activity, such as diagnosis, intervention, error or negligence), for example, the side-effects of urological surgeries like, prostatectomy, radiotherapy as part of prostate cancer treatment, post transurethral resection of the prostate
For example,
Hormonal causes:Hormonal triggers for ED are uncommon in young people but can include:
- hypogonadism
- thyroid
- klinefelter’s syndrome (KS)
- cryptorchidism
- antidepressants
- NSAIDs
- finasteride (Propecia)
- antiepileptics
- neuroleptics
- antihypertensives
- antipsychotics
- Beta-blockers – although these are only thought to be a minor contributor to ED and sexual dysfunction
- Drug abuse, including taking recreational drugs and opioids (which can cover the illegal drug heroin, synthetic opioids, such as fentanyl, and pain relievers available legally by prescription, codeine, morphine etc).
- Chronic alcohol abuse – can provoke vascular damages, that is, injury to the circulatory system, made up of vessels, arteries and veins that transport blood around your body. According to an animal study, chronic alcohol abuse is suspected to cause:
- loss of smooth corporal muscle tissue (smooth muscle fibres contribute to the rigidity and stability of the erect penis),
- early neuropathy (damage to nerves located outside the brain or spinal chord, usually resulting in numbness or weakness), and
- the direct alcoholic toxicity to the corporal endothelium (a thin membrane that lines penis blood vessels).
- loss of smooth corporal muscle tissue (smooth muscle fibres contribute to the rigidity and stability of the erect penis),
- Cigarette smoking
- Obesity – amongst a whole host of other modifiable risk factors that casually contribute to the development of ED, such as insomnia and snoring, obesity was also identified. In particular, genetically predicted body mass index (BMI), waist circumference, trunk fat mass, and whole body fat mass were found to increase the risk of ED. Meanwhile, a genetic tendency to have a higher body fat percentage was suggestively associated with an increased risk of ED.
- Limited or lack of physical exercise
- Cycling – although the part bicycle riding plays in ED remains controversial, a 2020 meta-analysis of 3,330 cyclists compared to 1,524 non-cycling participants indicated a significantly increased risk of ED in the cyclists. Researchers did, however, conclude that there was limited evidence that supports a positive correlation between cycling and ED when adjusting for age and several comorbidities (other conditions).
- Exposure to endocrine (hormonal) disrupters like pesticides – Despite age and experiencing things like obesity, diabetes and hypertension, for example, playing a part in ED prognosis, some studies suggest exposure to environmental contaminants could also be the reason for the rising trend in ED.
A study of 671 adult men, representing 28,949,379 adults after survey weighting, where approximately 37% of the participants were living with ED, found that smoking, diabetes, ageing, Mexican-American self-identification, and physical inactivity were associated with higher ED prevalence. However, they also discovered a possible role for organophosphate (OP) insecticides, particularly chlorpyrifos (the most commonly used OP in the U.S.) in the pathogenesis of ED, with the ED risk increasing with heightened exposure to the chemical. - Antiseptic mouthwashes – The molecule, nitric oxide (not be confused with laughing gas or nitrous oxide (N2O)) is key in getting and keeping an erection. As antiseptic mouthwashes eliminate bacteria in your mouth, this nitric oxide-generating pathway is abolished, which may result in nitric oxide-deficient conditions, potentially impacting erections. Indeed, short-term clinical trials have shown that antibacterial mouthwash deplete oral nitrate-reducing bacteria, and decrease systemic nitric oxide bioavailability – the ability of something to enter your circulation to have an effect.
Can erectile dysfunction be cured?
Although ageing, something we can’t help, is an important factor contributing to ED (as people age, cardiovascular diseases, hypertension, and other co-morbidities play an increasingly significant role in ED), there are several steps you can take, alongside seeing your GP as soon as possible, to prevent ED or reduce it.
As a bonus, many of these lifestyle changes that can help you optimise your penis and overall health, can also help minimise your risk of cardiovascular diseases – which are sadly one of the main causes of death and disability in the UK, with heart and circulatory diseases causing a quarter of UK deaths – more than 160,000 – each year, despite being largely preventable.
- Stop smoking, if you do; here are some supportive organisations to help. We mentioned above that COPD is a significant high risk factor of developing ED, regardless of age and the presence of other conditions. A main cause of COPD is smoking, so quitting can help control your COPD status if you have it, whilst there’s a strong association between the intensity of cigarette smoking and the degree of ED. This means even cutting down is likely to help alleviate ED symptoms.
- Embrace nourishing nutrition; discover what healthy meals look like here. Part of it, is avoiding the industrial trans fats found in fried, processed and commercially baked foods. Weaving protein into your breakfast can help you feel fuller for longer and minimise those sugary cravings. Ideas include eggs, adding nuts and seeds to your porridge, and tucking into lean meats or fish – this could be having last night’s leftovers (if it was healthy of course!).
Another element of healthily fuelling your body, is achieving good glycaemic control, which can help prevent hypertension, type 2 diabetes and obesity, all aforementioned ED causes. Low Glycaemic Index and low Glycaemic Load foods include, non-starchy veggies and fruit, such as asparagus, broccoli, spinach, apples, blueberries and pears and pulses, for example, lentils, kidney beans and chickpeas. Sugary foods like cakes, biscuits, sugary soft drinks (including fruit juices), some breakfast cereals and most white carbohydrates, for instance, bread, pasta and rice make up high glycaemic foods, which are best avoided or had as an occasional treat. - Move your body more; here are the five key areas to focus on and ideas to get you started. Muscle strengthening routines that include, for example, squats with weights sufficient enough to make 1-12 repetitions a challenge, bench press, leg press or bicep curl and muscle endurance exercises, for instance, muscle strengthening exercises but for more than 12 repetitions with lower weights or plank holding, can help prevent skeletal muscle mass loss, and therefore help prevent low testosterone levels, as covered above.
- Manage your alcohol intake, with these practical tips.
Should you or someone in your life be concerned about your alcohol intake or you’re struggling to reduce your alcohol consumption, contact your GP for support or reach out to a local alcohol support service, for instance, Alcohol Change UK for non-judgemental advice.
If you’re overweight or obese, a combination of the above can contribute to you maintaining a healthy weight and reducing visceral fat wrapped around your major organs – which helps cut your cardiovascular disease risk.
- Minimise stress; we can sometimes feel like this is easier said than done, or buy into the stories we tell ourselves that we don’t have time to prioritise our own wellbeing, but making sure we do is essential. This will look different for different people, but breathing exercises, yoga, finding a hobby like painting, or playing a musical instrument can all help. Identify what works for you.
- Seek support; from your GP if you’re experiencing medication side-effects and or from various organisations like Mental Health Foundation, CALM, and Men’s Health Forum, which can offer practical help and understanding, should you be struggling with poor mental health. You’re not alone. Our resources on anxiety and depression may also offer some practical steps you can take to reduce these feelings.
- Switch to a natural mouthwash; your and your partner can even make your own, fairly quickly. Avoid using salt mouthwash in the long-term as doing so can create its own issues.
Never rely on, for example, Viagra alone and hope the problem will go away as you may be putting your health and life at risk. Instead, promptly consult your healthcare provider if:
– you’re experiencing ED, even if you don’t think it’s due to a serious underlying condition. With it often being potential early sign of cardiovascular diseases, diabetes, and / or depression, and neurological conditions, your GP can rule out the conditions or provide support on which lifestyle changes can minimise or prevent the potential progression to more serious conditions.
They can also provide further tests and investigations to determine the cause and what treatments may be needed.
– you’re at all concerned, as there can be many other potential signs of the conditions highlighted above, besides ED.
Keeping an eye on your own or and/or your partner’s penis health, as well as incorporating the above lifestyle behaviours, can combine to help prevent you from experiencing ED and cardiovascular diseases.
Since monitoring yours or your partner’s erections is simple and quick observation and costs nothing, what’s the harm in doing it? It could cost you more if you don’t…
Our free Evergreen Life app can help support you to live a healthy lifestyle.
Reviewed by:
Anna Keeble MA BA Head of Content and Wellbeing Expert
Dr Claire Marie Thomas MRCGP DFSRH DTMH DipNLP MBChB BMedSci Medical Expert
- Alcohol Change UK (n.d.). Alcohol harms. Time for change. [online] Alcohol Change UK. Available here.
- Alwaal, A., Awad, M., Boggs, N., Kuzbel, J. and Snoad, B. (2020). Sexual Health Inventory for Men Questionnaire as a Screening Method for Erectile Dysfunction in a General Urology Clinic. Sexual Medicine, 8(4), pp.660–663. Available here.
- Antonio L, Wu FCW, Moors H, Matheï C, Huhtaniemi IT, Rastrelli G, Dejaeger M, O’Neill TW, Pye SR, Forti G, Maggi M, Casanueva FF, Slowikowska-Hilczer J, Punab M, Tournoy J, Vanderschueren D; EMAS Study Group. (2022). Erectile dysfunction predicts mortality in middle-aged and older men independent of their sex steroid status. Age Ageing, 51(4): afac094. Available here.
- Beyond Pesticides. (2023). Common Pesticides Linked to Erectile Dysfunction in Younger Males. [online] Children’s Health Defense. Available here. [Accessed 8 Dec. 2023].
- Blot, S. (2020). Antiseptic mouthwash, the nitrate–nitrite–nitric oxide pathway, and hospital mortality: a hypothesis generating review. Intensive Care Medicine, 47(1), pp.28-38. Available here.
- British Heart Foundation. (2023). Facts and Figures. [online] British Heart Foundation. Available here.
- Chen, C.-M., Tsai, M.-J., Wei, P.-J., Su, Y.-C., Yang, C.-J., Wu, M.-N., Hsu, C.-Y., Hwang, S.-J., Chong, I.-W. and Huang, M.-S. (2015). Erectile Dysfunction in Patients with Sleep Apnea – A Nationwide Population-Based Study. PLOS ONE, 10(7), p.e0132510 Available here.
- Diabetes UK (n.d.). Diabetes and sexual problems – in men. [online] Diabetes UK. Available here. [Accessed 12 Dec. 2023].
- Diabetes UK (2021). What is HbA1c? [online] Diabetes UK. Available here.
- Dong, J.-Y., Zhang, Y.-H. and Qin, L.-Q. (2011). Erectile Dysfunction and Risk of Cardiovascular Disease. Journal of the American College of Cardiology, 58(13), pp.1378–1385. Available here.
- Emanu, J.C., Avildsen, I.K. and Nelson, C.J. (2016). Erectile dysfunction after radical prostatectomy. Current Opinion in Supportive & Palliative Care, 10(1), pp.102–107. Available here.
- Gan, Z.S., Ehlers, M.E., Lin, F.-C., Wright, S.T., Figler, B.D. and Coward, R.M. (2020). Systematic Review and Meta-Analysis of Cycling and Erectile Dysfunction. Sexual Medicine Reviews, 9(2), pp.304-311. Available here.
- Glover, F., Mehta, A., Richardson, M., Muncey, W., Francesco Del Giudice, Belladelli, F., N. Seranio and Eisenberg, M.L. (2023). Investigating the prevalence of erectile dysfunction among men exposed to organophosphate insecticides. Journal of Endocrinological Investigation. Available here.
- Goodale, T., Sadhu, A., Petak, S. and Robbins, R. (2017). Testosterone and the Heart. Methodist DeBakey Cardiovascular Journal, 13(2), pp.68–72. Available here.
- Hill, M. and Bordoni, B. (2023). Hyperlipidemia. [online] StatPearls [Internet]. Available here.
- Hotta, Y., Kataoka, T., Mori, T. and Kimura, K. (2020). Review of a Potential Novel Approach for Erectile Dysfunction: Light-Controllable Nitric Oxide Donors and Nanoformulations. Sexual Medicine Reviews, [online] 8(2), pp.297–302. Available here.
- Hoyos, C.M., Melehan, K.L., Phillips, C.L., Grunstein, R.R. and Liu, P.Y. (2015). To ED or not to ED – Is erectile dysfunction in obstructive sleep apnea related to endothelial dysfunction? Sleep Medicine Reviews, 20, pp.5–14. Available here.
- Hunt, A.A., Choudhury, K.R., Nukala, V., Nolan, M.W., Ahmad, A., Ashcraft, K.A. and Koontz, B.F. (2021). Risk of erectile dysfunction after modern radiotherapy for intact prostate cancer. Prostate Cancer and Prostatic Diseases, [online] 24(1), pp.128–134. Available here.
- Jahangiry, L., Farhangi, M.A. and Rezaei, F. (2017). Framingham risk score for estimation of 10-years of cardiovascular diseases risk in patients with metabolic syndrome. Journal of Health, Population and Nutrition, 36(1). Available here.
- Joshipura, K., Muñoz-Torres, F., Fernández-Santiago, J., Patel, R.P. and Lopez-Candales, A. (2019). Over-the-counter mouthwash use, nitric oxide and hypertension risk. Blood Pressure, 29(2), pp.103–112. Available here.
- Ko DT, Hebert PR, Coffey CS, Sedrakyan A, Curtis JP, Krumholz HM. Beta-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA. 2002 Jul 17;288(3):351-7. Available here.
- Kouidrat, Y., Pizzol, D., Cosco, T., Thompson, T., Carnaghi, M., Bertoldo, A., Solmi, M., Stubbs, B. and Veronese, N. (2017). High prevalence of erectile dysfunction in diabetes: a systematic review and meta-analysis of 145 studies. Diabetic Medicine, 34(9), pp.1185–1192. Available here.
- Larson TR. Current treatment options for benign prostatic hyperplasia and their impact on sexual function. Urology. 2003 Apr;61(4):692-8. Available here.
- Li, S., Song, J.-M., Zhang, K. and Zhang, C.-L. (2021). A Meta-Analysis of Erectile Dysfunction and Alcohol Consumption. Urologia Internationalis, 105(11-12), pp.969–985. Available here.
- Ludwig, W. and Phillips, M. (2014). Organic Causes of Erectile Dysfunction in Men Under 40. Urologia Internationalis, 92(1), pp.1–6. Available here.
- Maggi, M., Rastrelli, G. and Corona, G. (2020). Both comorbidity burden and low testosterone can explain symptoms and signs of testosterone deficiency in men consulting for sexual dysfunction. Asian Journal of Andrology, 22(3), p.265-273. Available here.
- Mazzilli, R., Angeletti, G., Olana, S., Delfino, M., Zamponi, V., Rapinesi, C., Del Casale, A., Kotzalidis, G.D., Elia, J., Callovini, G., Girardi, P. and Mazzilli, F. (2018). Erectile dysfunction in patients taking psychotropic drugs and treated with phosphodiesterase-5 inhibitors. Archivio Italiano di Urologia e Andrologia, 90(1), p.44. Available here.
- Marchesi, S., Lupattelli, G., Schillaci, G., Pirro, M., Siepi, D., Roscini, A.R., Pasqualini, L. and Mannarino, E. (2000). Impaired flow-mediated vasoactivity during post-prandial phase in young healthy men. Atherosclerosis, [online] 153(2), pp.397–402. Available here.
- Meirelles, R.J. de A., Lizarte Neto, F.S., Cirino, M.L. de A., Novais, P.C., Gula, I.S., Silva, J.P. da, Tazzima, M. de F.G.S., Fazan, V.P.S., Durand, M.T., Tirapelli, D.P. da C., Carvalho, C.A.M. de, Schimming, B.C., Molina, C.A.F., Tucci Junior, S. and Tirapelli, L.F. (2020). Morphological and molecular analysis of apoptosis in the corpus cavernosum of rats submitted to a chronic alcoholism model. Acta Cirúrgica Brasileira, [online] 35 (3), p.e202000305. Available here.
- Mori, T., Hotta, Y., Nakamura, D., R. Yahagi, Kataoka, T. and Kimura, K. (2021). Enhancement of the RhoA/Rho kinase pathway is associated with stress‐related erectile dysfunction in a restraint water immersion stress model. Physiological Reports, 9(20), p.e15064. Available here.
- Nathoo NA, Etminan M, Mikelberg FS. Association between glaucoma, glaucoma therapies, and erectile dysfunction. J Glaucoma. 2015 Feb;24(2):135-7. Available here.
- NHS (2019). Atherosclerosis (arteriosclerosis). [online] NHS. Available here.
- NHS (2022). Cardiovascular disease. [online] NHS. Available here.
- NHS (2022). The ‘male menopause’. [online] NHS. Available here.
- NHS (2023). Chronic Obstructive Pulmonary Disease (COPD). [online] NHS. Available here.
- NHS (2023). Erectile dysfunction (impotence). [online] NHS. Available here.
- NHS (2023). What is type 2 diabetes? [online] NHS. Available here.
- NHS inform (2023). Erectile dysfunction. [online] Available here.
- Novo, S., Iacona, R., Bonomo, V., Evola, V., Corrado, E., Di Piazza, M., Novo, G. and Pavone, C. (2015). Erectile dysfunction is associated with low total serum testosterone levels and impaired flow-mediated vasodilation in intermediate risk men according to the framingham risk score. Atherosclerosis, 238(2), pp.415–419. Available here.
- Pourmand, G., Alidaee, M.R., Rasuli, S., Maleki, A. and Mehrsai, A. (2004). Do cigarette smokers with erectile dysfunction benefit from stopping?: a prospective study. BJU International, 94(9), pp.1310–1313. Available here.
- Rajfer, J. (2000). Relationship Between Testosterone and Erectile Dysfunction. Reviews in Urology, [online] 2(2), pp.122–128. Available here.
- Razdan S, Greer AB, Patel A, Alameddine M, Jue JS, Ramasamy R. Effect of prescription medications on erectile dysfunction. Postgrad Med J. 2018 Mar;94(1109):171-178. Available here.
- Rubin, R.S. (2023.). The Easy Way to Talk About Penises. [online] Medscape. Available here. [Accessed 20 Dec. 2023].
- Shamloul, R. and Ghanem, H. (2013). Erectile dysfunction. The Lancet, 381(9861), pp.153–165. Available here.
- Simply Dental. (2023). 9 natural mouthwash alternatives to cure bad breath. [online] Available here. [Accessed 8 Dec. 2023]
- Sooriyamoorthy, T. and Leslie, S.W. (2023). Erectile Dysfunction. [online] StatPearls [Inernet]. Available here.
- Te Chun Shen, Wen Chi Chen, Lin, C.-L., Chen, C.-H., Chih Yen Tu, Te Chun Hsia, Chuen Ming Shih, Hsu, W.-H. and Sung, F.-C. (2015). The Risk of Erectile Dysfunction in Chronic Obstructive Pulmonary Disease. Medicine, 94(14), pp.e448. Available here.
- Tsujimura, A., Hiramatsu, I., Aoki, Y., Shimoyama, H., Mizuno, T., Nozaki, T., Shirai, M., Kobayashi, K., Kumamoto, Y. and Horie, S. (2017). Atherosclerosis is associated with erectile function and lower urinary tract symptoms, especially nocturia, in middle-aged men. Prostate International, 5(2), pp.65–69. Available here.
- Wan, Y., Piao, L., Xu, S., Inoue, A., Meng, X., Lei, Y., Huang, Z., Wang, H., Yue, X., Shi, G., Masafumi Kuzuya and Cheng, X. (2023). Cathepsin S deficiency improves muscle mass loss and dysfunction via the modulation of protein metabolism in mice under pathological stress conditions. The FASEB Journal, 37(8), p.e23086. Available here.
- Xiong, Y., Zhang, F., Zhang, Y., Wang, W., Ran, Y., Wu, C., Zhu, S., Qin, F. and Yuan, J. (2023). Insights into modifiable risk factors of erectile dysfunction, a wide-angled Mendelian Randomization study. Journal of Advanced Research, [online] pp.S2090-1232(23)00147-9. Available here.
- Yuki, A., Otsuka, R., Kozakai, R., Kitamura, I., Okura, T., Ando, F. and Shimokata, H. (2013). Relationship between Low Free Testosterone Levels and Loss of Muscle Mass. Scientific Reports, 3(1), p. 1818. Available here.
- Zhao, B., Hong, Z., Wei, Y., Yu, D., Xu, J. and Zhang, W. (2019). Erectile Dysfunction Predicts Cardiovascular Events as an Independent Risk Factor: A Systematic Review and Meta-Analysis. The Journal of Sexual Medicine, 16(7), pp.1005–1017. Available here.



